Southernscripts.net Prior Authorization Form
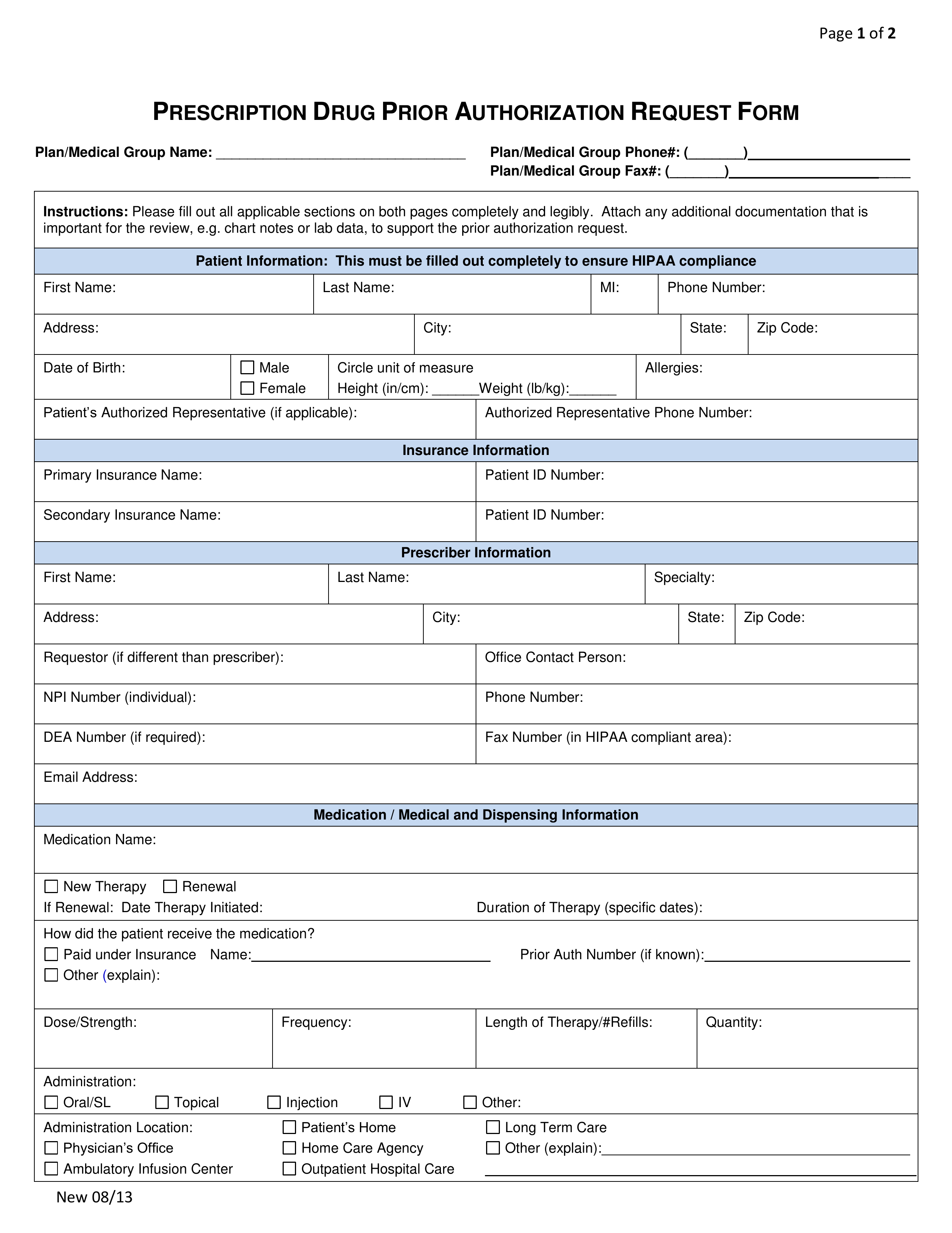
Southernscripts.net Prior Authorization Form - Web we would like to show you a description here but the site won’t allow us. Web we would like to show you a description here but the site won’t allow us. Web open the southern scripts mobile app and login using your credentials. Web we are improving the member portal! Web the submission of this rx claim form, for you and/or dependents, authorizes the release of all information to the plan sponsor, administrator, and/or pharmacy benefit manager i accept. Members must use the exact name issued on their id card to complete registration and login authentication. If you do not have credentials, please select the button labeled create your account. Web prior authorization appeal form; Name of drug/medication strength of the drug (example 5 mg) quantity being prescribed days supply for medical services: Adobe reader or any alternative for windows or macos are required to.
Web we would like to show you a description here but the site won’t allow us. Name of drug/medication strength of the drug (example 5 mg) quantity being prescribed days supply for medical services: Web prior authorization appeal form; I also confirm that the patient, for whom this claim is made, had coverage at the time the. Web open the southern scripts mobile app and login using your credentials. Members must use the exact name issued on their id card to complete registration and login authentication. Web no additional fees for standard pbm services, such as prior authorizations, step therapy, and data reporting. Select more from the bottom menu navigation. Web this information can be obtained by contacting your prescribing physician. I certify that the information on this form is correct.
Select more from the bottom menu navigation. Web we would like to show you a description here but the site won’t allow us. I certify that the information on this form is correct. Adobe reader or any alternative for windows or macos are required to. Web the submission of this rx claim form, for you and/or dependents, authorizes the release of all information to the plan sponsor, administrator, and/or pharmacy benefit manager i accept. Web open the southern scripts mobile app and login using your credentials. Web we are improving the member portal! If you do not have credentials, please select the button labeled create your account. Description of service start date of service end date of service service code if available (hcpcs/cpt) new prior authorization Members must use the exact name issued on their id card to complete registration and login authentication.

Medicare Generation Rx Prior Authorization Form Form Resume
I certify that the information on this form is correct. Web we are improving the member portal! Name of drug/medication strength of the drug (example 5 mg) quantity being prescribed days supply for medical services: Members must use the exact name issued on their id card to complete registration and login authentication. I also confirm that the patient, for whom.
Bcbs Prior Authorization Form Alabama Form Resume Examples 5xm1e7r3rL
If you do not have credentials, please select the button labeled create your account. Name of drug/medication strength of the drug (example 5 mg) quantity being prescribed days supply for medical services: Web prior authorization appeal form; Web no additional fees for standard pbm services, such as prior authorizations, step therapy, and data reporting. Select more from the bottom menu.

Oscar Prior Authorization form Fresh Free Health Net Prior Rx
Web no additional fees for standard pbm services, such as prior authorizations, step therapy, and data reporting. If you do not have credentials, please select the button labeled create your account. Description of service start date of service end date of service service code if available (hcpcs/cpt) new prior authorization Web prior authorization appeal form; Name of drug/medication strength of.
Aarp Prior Authorization Form Form Resume Examples dP9lDOk9RD
Web open the southern scripts mobile app and login using your credentials. I certify that the information on this form is correct. Adobe reader or any alternative for windows or macos are required to. Web this information can be obtained by contacting your prescribing physician. Web the submission of this rx claim form, for you and/or dependents, authorizes the release.
Bcbs Prior Authorization Form Ohio Form Resume Examples 9lV8N5A30o
Name of drug/medication strength of the drug (example 5 mg) quantity being prescribed days supply for medical services: Members must use the exact name issued on their id card to complete registration and login authentication. If you do not have credentials, please select the button labeled create your account. Web no additional fees for standard pbm services, such as prior.
Key.covermymeds Prior Authorization Form Form Resume Examples
Members must use the exact name issued on their id card to complete registration and login authentication. Web we are improving the member portal! If you do not have credentials, please select the button labeled create your account. Description of service start date of service end date of service service code if available (hcpcs/cpt) new prior authorization Web the submission.
Free SAVRX Prior (Rx) Authorization Form PDF eForms
Description of service start date of service end date of service service code if available (hcpcs/cpt) new prior authorization Web no additional fees for standard pbm services, such as prior authorizations, step therapy, and data reporting. Adobe reader or any alternative for windows or macos are required to. Select more from the bottom menu navigation. Web prior authorization appeal form;
Bcbs Prior Auth Forms Florida Form Resume Examples A4kn4J95jG
Description of service start date of service end date of service service code if available (hcpcs/cpt) new prior authorization Web we would like to show you a description here but the site won’t allow us. Name of drug/medication strength of the drug (example 5 mg) quantity being prescribed days supply for medical services: Web open the southern scripts mobile app.
Sample Caremark Prior Authorization Form 8+ Free Documents in PDF
Description of service start date of service end date of service service code if available (hcpcs/cpt) new prior authorization I certify that the information on this form is correct. Web we would like to show you a description here but the site won’t allow us. Web we are improving the member portal! Adobe reader or any alternative for windows or.

Bcbs Prior Authorization Form Alabama Form Resume Examples 5xm1e7r3rL
I also confirm that the patient, for whom this claim is made, had coverage at the time the. If you do not have credentials, please select the button labeled create your account. Name of drug/medication strength of the drug (example 5 mg) quantity being prescribed days supply for medical services: Web we would like to show you a description here.
Select More From The Bottom Menu Navigation.
Web open the southern scripts mobile app and login using your credentials. Web this information can be obtained by contacting your prescribing physician. Web we would like to show you a description here but the site won’t allow us. Members must use the exact name issued on their id card to complete registration and login authentication.
Web No Additional Fees For Standard Pbm Services, Such As Prior Authorizations, Step Therapy, And Data Reporting.
Web the submission of this rx claim form, for you and/or dependents, authorizes the release of all information to the plan sponsor, administrator, and/or pharmacy benefit manager i accept. Web we would like to show you a description here but the site won’t allow us. Web we are improving the member portal! If you do not have credentials, please select the button labeled create your account.
I Also Confirm That The Patient, For Whom This Claim Is Made, Had Coverage At The Time The.
I certify that the information on this form is correct. Adobe reader or any alternative for windows or macos are required to. Name of drug/medication strength of the drug (example 5 mg) quantity being prescribed days supply for medical services: Web prior authorization appeal form;