Aetna Specialty Pharmacy Prior Authorization Form
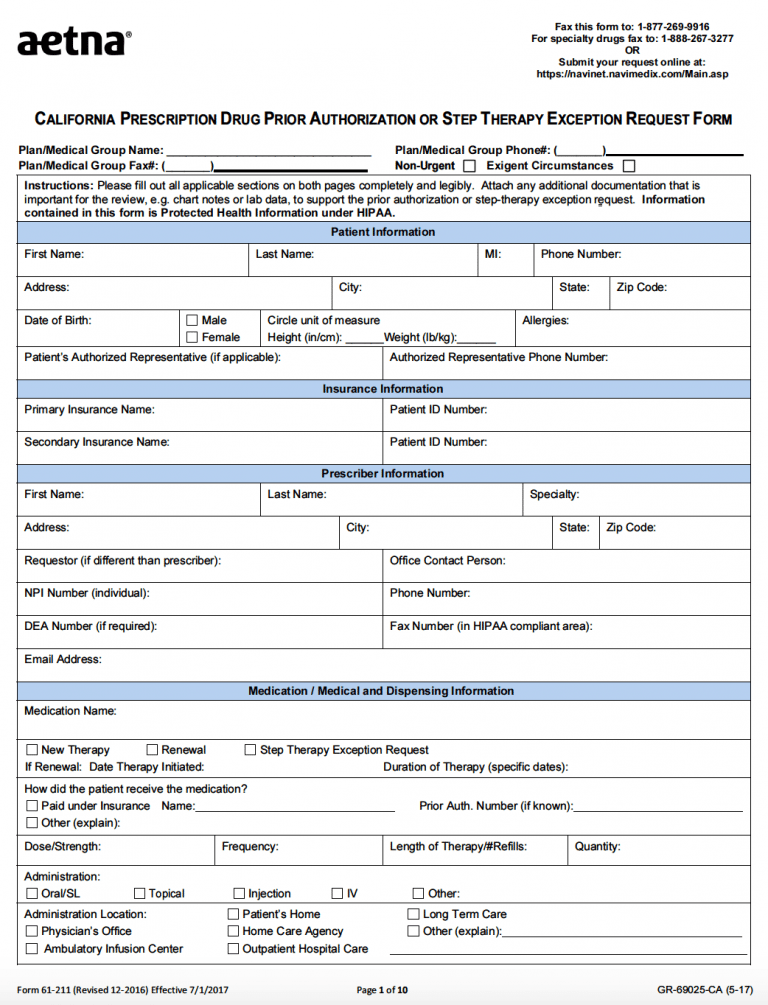
Aetna Specialty Pharmacy Prior Authorization Form - Pharmacy prior authorization forms acromegaly agents. Web aetna precertification notification phone: (all fields must be completed and legible for precertification review.) please use medicare request form patient first name. Web aetna specialty pharmacy forms. Web we have several ways for you to fill a prescription through the network specialty pharmacy. Web pdf/ua accessible pdf aetna rx medical exceptio prior authrizatio precertifcation request for prescription medications. General medication request form (pdf,1 mb) crohn's/ulcerative colitis medication request form (pdf, 349 kb) enzyme replacement medication request form (pdf, 541 kb) growth hormone medication request form (pdf, 239 kb) hemophilia medication request form (pdf, 591 kb) Start date continuation of therapy: Page 1 of 2 pharmacy prior authorization request form 6. You can find the related pa request forms here.
Start date continuation of therapy: Pharmacy prior authorization forms acromegaly agents. Web aetna specialty pharmacy forms. (all fields must be completed and legible for precertification review.) please use medicare request form patient first name. For medicare advantage part b: Web pharmacy prior authorization request form do not copy for future use. You can find the related pa request forms here. Page 1 of 2 pharmacy prior authorization request form 6. Office notes, labs, and medical testing relevant to the request that show medical justification are required. Click on the drug name to download the prior authorization request form.
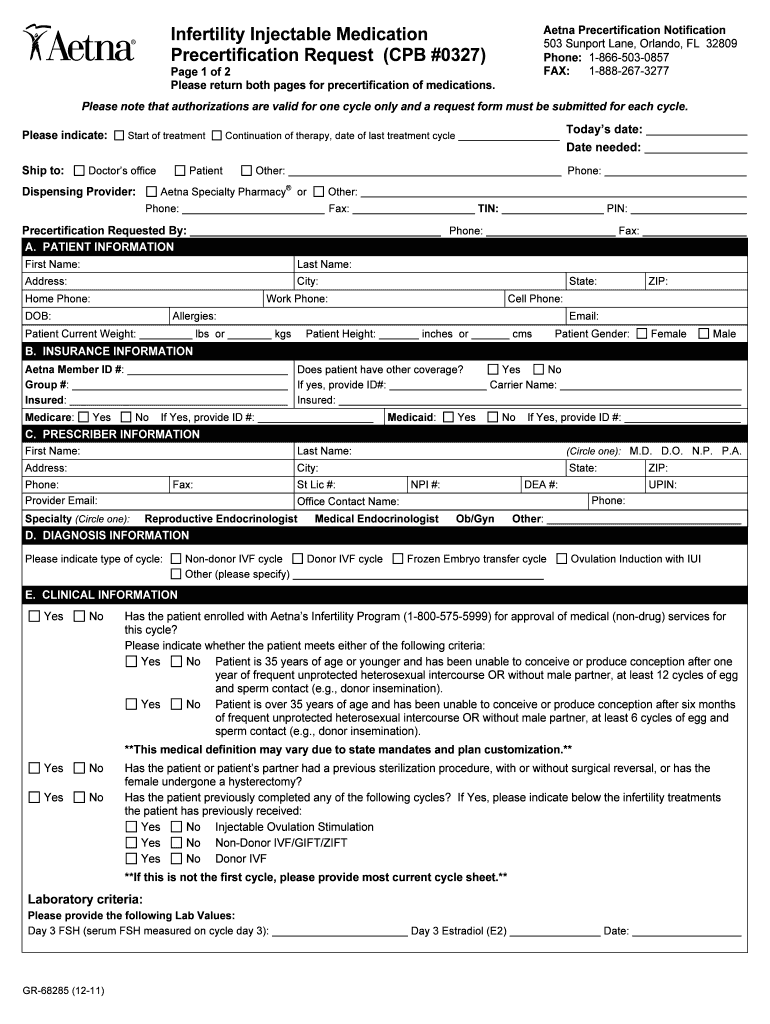
These are fax forms for drugs in our prior authorization program. For a new prescription, your doctor can: Office notes, labs, and medical testing relevant to the request that show medical justification are required. Start date continuation of therapy: You can find the related pa request forms here. General medication request form (pdf,1 mb) crohn's/ulcerative colitis medication request form (pdf, 349 kb) enzyme replacement medication request form (pdf, 541 kb) growth hormone medication request form (pdf, 239 kb) hemophilia medication request form (pdf, 591 kb) Web specialty medication precertification request aetna precertification notification phone: Web aetna precertification notification phone: Submit your initial request on availity with the authorization (precertification) add transaction. Pharmacy prior authorization forms acromegaly agents.

20192022 Form Aetna GR690251 CO Fill Online, Printable, Fillable
Web pharmacy prior authorization request form do not copy for future use. Click on the drug name to download the prior authorization request form. Web aetna specialty pharmacy forms. Submit your initial request on availity with the authorization (precertification) add transaction. You can find the related pa request forms here.

Aetna Prior Authorization Form Medical Record Health Sciences
Then complete a short questionnaire, if asked, to. Page 1 of 2 pharmacy prior authorization request form 6. Web aetna specialty pharmacy forms. Office notes, labs, and medical testing relevant to the request that show medical justification are required. General medication request form (pdf,1 mb) crohn's/ulcerative colitis medication request form (pdf, 349 kb) enzyme replacement medication request form (pdf, 541.

From This Point. Forward. Aetna "Specialty" Pharmacy
Pharmacy prior authorization forms acromegaly agents. These are fax forms for drugs in our prior authorization program. General medication request form (pdf,1 mb) crohn's/ulcerative colitis medication request form (pdf, 349 kb) enzyme replacement medication request form (pdf, 541 kb) growth hormone medication request form (pdf, 239 kb) hemophilia medication request form (pdf, 591 kb) Web aetna precertification notification phone: Web.
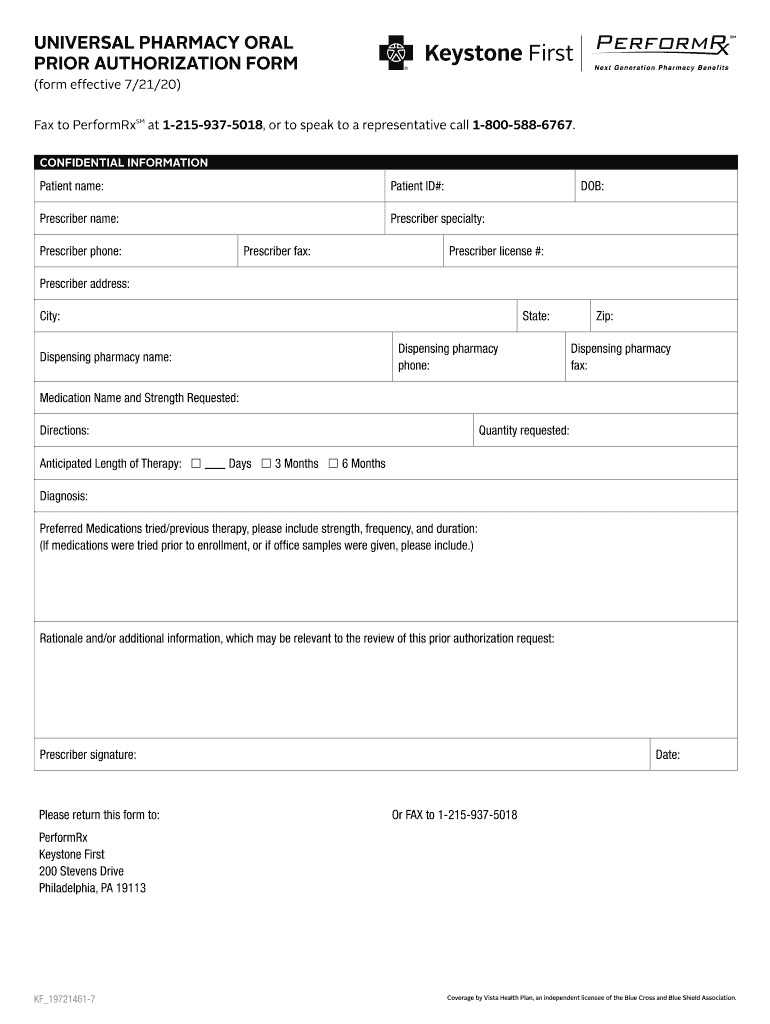
Keystone First Universal Pharmacy Oral Prior Authorization Form 2020
You can find the related pa request forms here. Pharmacy prior authorization forms acromegaly agents. Then complete a short questionnaire, if asked, to. For a new prescription, your doctor can: Web we have several ways for you to fill a prescription through the network specialty pharmacy.
Aetna Medicare Waiver Of Liability Form Form Resume Examples
Office notes, labs, and medical testing relevant to the request that show medical justification are required. These are fax forms for drugs in our prior authorization program. Web we have several ways for you to fill a prescription through the network specialty pharmacy. Web pdf/ua accessible pdf aetna rx medical exceptio prior authrizatio precertifcation request for prescription medications. Start date.
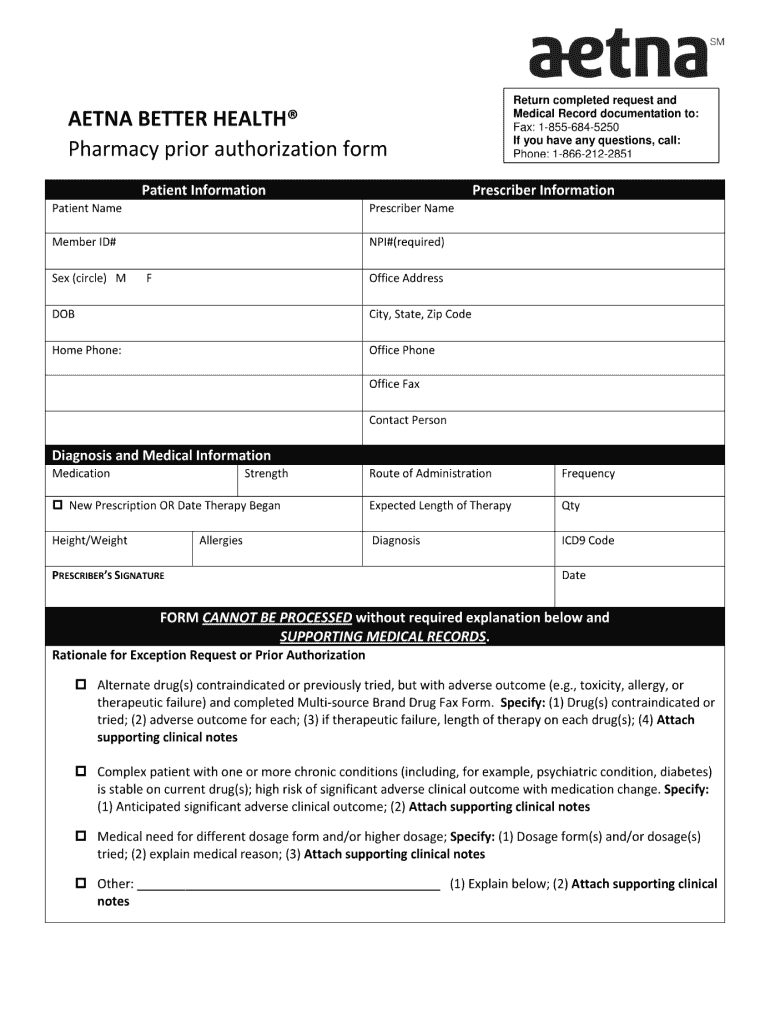
Aetna Specialty Pharmacy Prior Authorization Form PharmacyWalls
Click on the drug name to download the prior authorization request form. Start date continuation of therapy: General medication request form (pdf,1 mb) crohn's/ulcerative colitis medication request form (pdf, 349 kb) enzyme replacement medication request form (pdf, 541 kb) growth hormone medication request form (pdf, 239 kb) hemophilia medication request form (pdf, 591 kb) Then complete a short questionnaire, if.

نموذج خطاب توصية شخصي مجاني (لصديق)
(all fields must be completed and legible for precertification review.) please use medicare request form patient first name. Web aetna specialty pharmacy forms. General medication request form (pdf,1 mb) crohn's/ulcerative colitis medication request form (pdf, 349 kb) enzyme replacement medication request form (pdf, 541 kb) growth hormone medication request form (pdf, 239 kb) hemophilia medication request form (pdf, 591 kb).
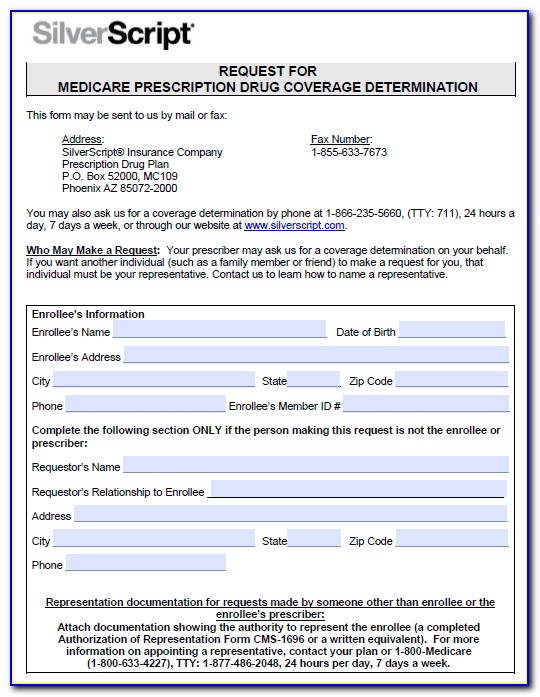
Medicare Part D Medco Prior Authorization Form Printable
Start date continuation of therapy: Web aetna precertification notification phone: General medication request form (pdf,1 mb) crohn's/ulcerative colitis medication request form (pdf, 349 kb) enzyme replacement medication request form (pdf, 541 kb) growth hormone medication request form (pdf, 239 kb) hemophilia medication request form (pdf, 591 kb) Web we have several ways for you to fill a prescription through the.
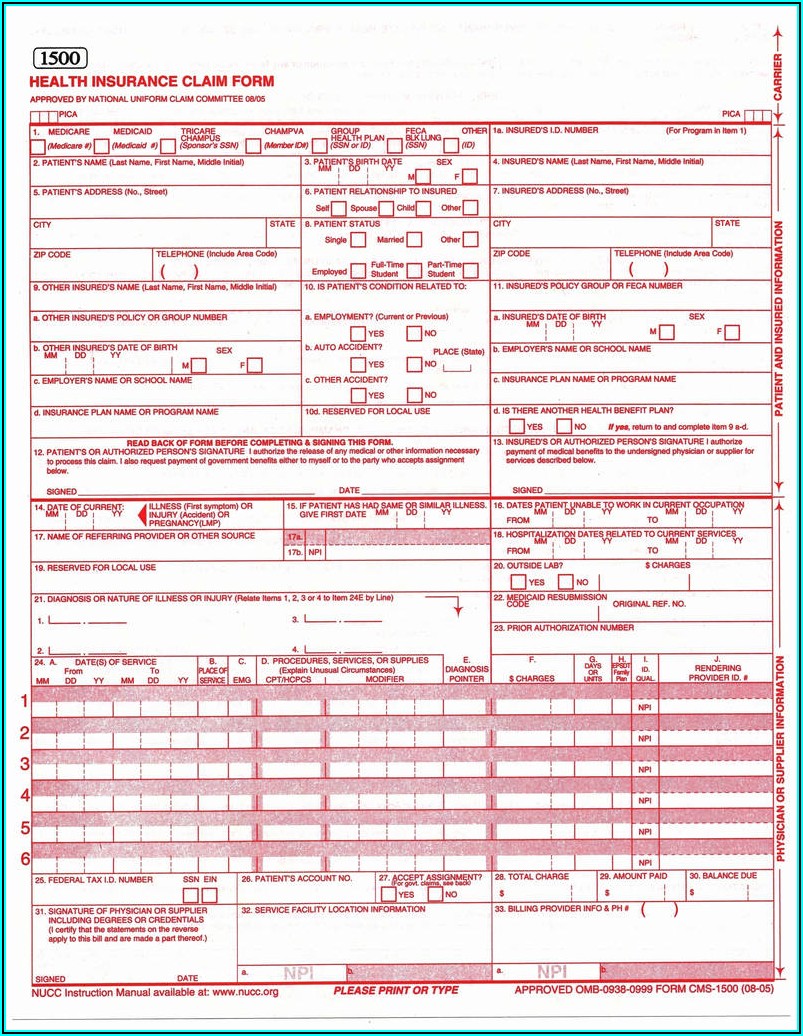
Free AETNA Prior Prescription (Rx) Authorization Form PDF
Start date continuation of therapy: Then complete a short questionnaire, if asked, to. Web pdf/ua accessible pdf aetna rx medical exceptio prior authrizatio precertifcation request for prescription medications. Web specialty medication precertification request aetna precertification notification phone: Web aetna precertification notification phone:
Precertification Aetna Sample Fill Online, Printable Fill Out and
Web pdf/ua accessible pdf aetna rx medical exceptio prior authrizatio precertifcation request for prescription medications. Submit your initial request on availity with the authorization (precertification) add transaction. Office notes, labs, and medical testing relevant to the request that show medical justification are required. Start date continuation of therapy: Pharmacy prior authorization forms acromegaly agents.
Then Complete A Short Questionnaire, If Asked, To.
Web pharmacy prior authorization request form do not copy for future use. For medicare advantage part b: Web pdf/ua accessible pdf aetna rx medical exceptio prior authrizatio precertifcation request for prescription medications. Click on the drug name to download the prior authorization request form.
Pharmacy Prior Authorization Forms Acromegaly Agents.
Web aetna specialty pharmacy forms. Web aetna precertification notification phone: Office notes, labs, and medical testing relevant to the request that show medical justification are required. Start date continuation of therapy:
Web We Have Several Ways For You To Fill A Prescription Through The Network Specialty Pharmacy.
(all fields must be completed and legible for precertification review.) please use medicare request form patient first name. Web specialty medication precertification request aetna precertification notification phone: You can find the related pa request forms here. These are fax forms for drugs in our prior authorization program.
For A New Prescription, Your Doctor Can:
General medication request form (pdf,1 mb) crohn's/ulcerative colitis medication request form (pdf, 349 kb) enzyme replacement medication request form (pdf, 541 kb) growth hormone medication request form (pdf, 239 kb) hemophilia medication request form (pdf, 591 kb) Submit your initial request on availity with the authorization (precertification) add transaction. Page 1 of 2 pharmacy prior authorization request form 6.