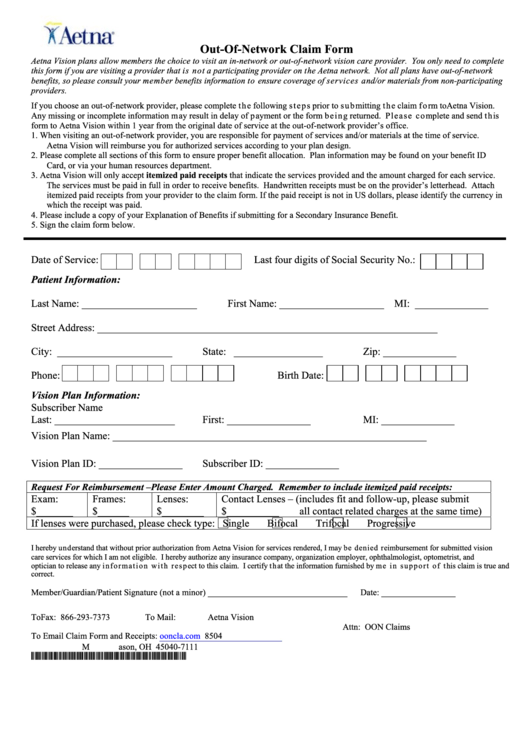
Aetna Vision Out Of Network Claim Form
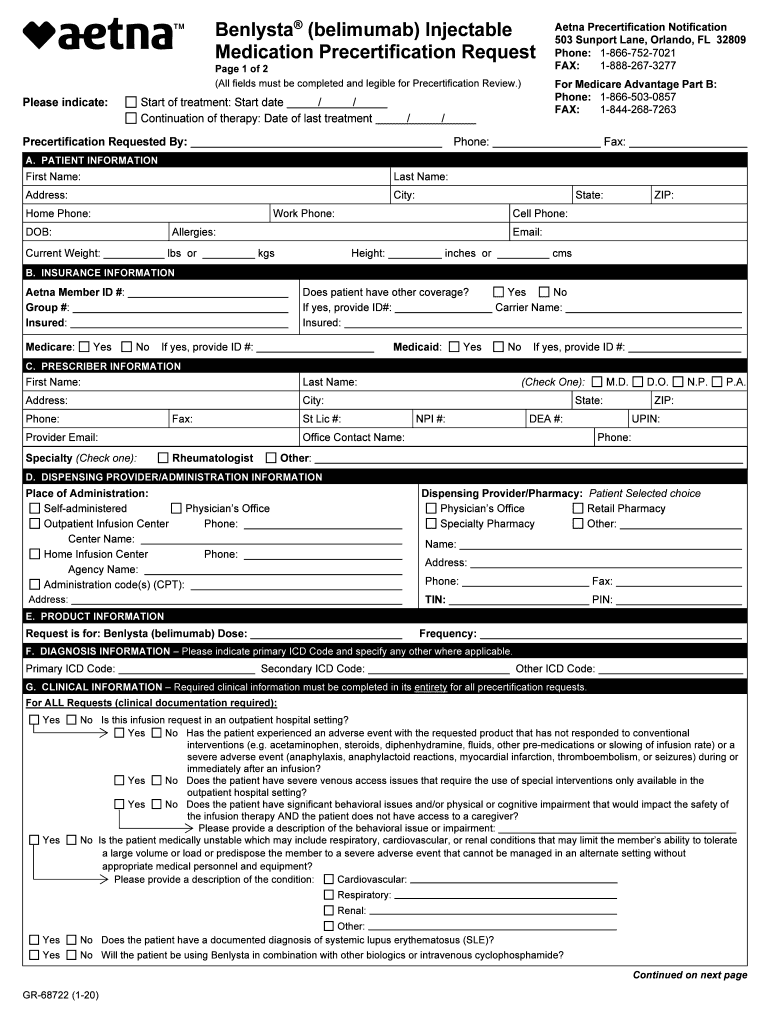
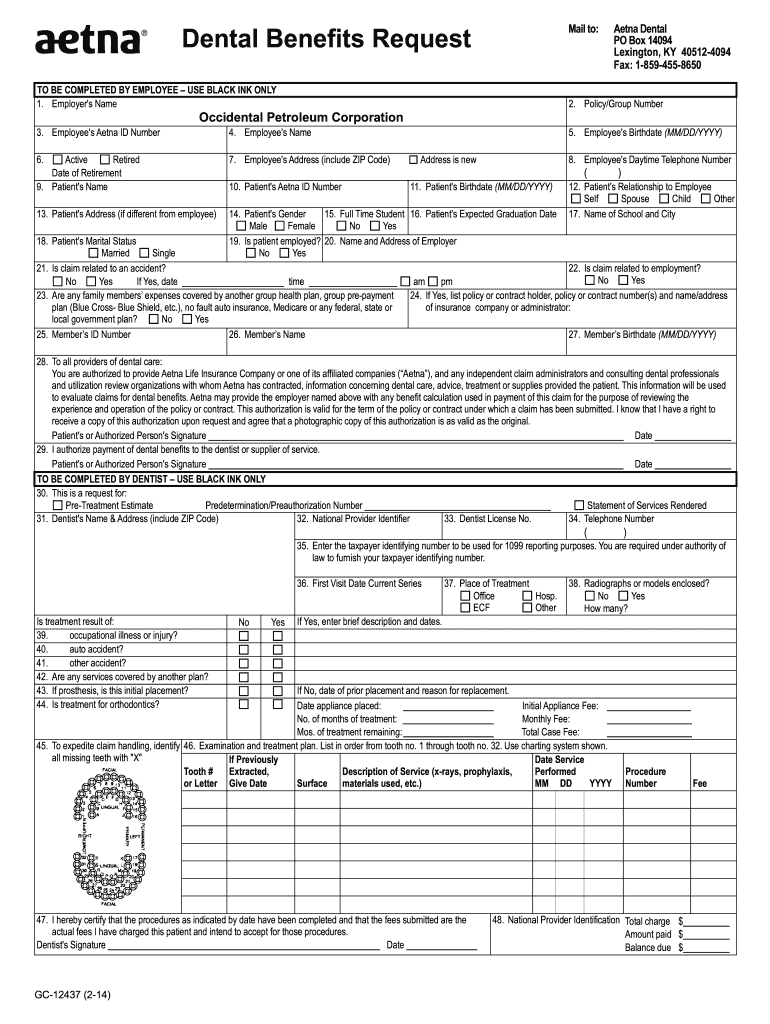
Aetna Vision Out Of Network Claim Form - Web watch newsmax live for the latest news and analysis on today's top stories, right here on facebook. Go green and get paid. Patient and subscriber information last name first name date of birth street address city state zip. Fill out this form if you’re asking for a medical, dental, vision, hearing, or vaccine reimbursement and you paid a doctor, healthcare professional, or. Click below to complete an electronic 2. If you don't receive an email in the next. Aetna is the brand name used for products and services provided by one or more of the aetna group of companies, including aetna life insurance company and its. Complete and return the claim form. Web for complete terms and conditions, review the claim form. Fill out this form if you paid a provider for covered medical, dental, vision, hearing or vaccination services and want to request.
Click below to complete an electronic 2. Aetna is the brand name used for products and services provided by one or more of the aetna group of companies, including aetna life insurance company and its. You can now submit your form online or. Web this form can be used to submit a claim for medical, dental, vision, or pharmaceutical services. Complete and return the claim form. Web watch newsmax live for the latest news and analysis on today's top stories, right here on facebook. If you're filing a claim for more than one person, a separate form is needed for. Fill out this form if you paid a provider for covered medical, dental, vision, hearing or vaccination services and want to request. Web explore claims options tools that save you time and money eras, efts and electronic eobs receive payments directly to your account. Web you can now submit your form online or by mail:
Web for complete terms and conditions, review the claim form. Web explore claims options tools that save you time and money eras, efts and electronic eobs receive payments directly to your account. Click below to complete an electronic 2. Web you can now submit your form online or by mail: Go green and get paid. If you don't receive an email in the next. You can now submit your form online or. Fill out this form if you’re asking for a medical, dental, vision, hearing, or vaccine reimbursement and you paid a doctor, healthcare professional, or. Web when to use this form? Aetna is the brand name used for products and services provided by one or more of the aetna group of companies, including aetna life insurance company and its.
Aetna Vision Preferred℠ App for iPhone Free Download Aetna Vision
Go green and get paid. Click below to complete an electronic 2. Web you can now submit your form online or by mail: Web this form can be used to submit a claim for medical, dental, vision, or pharmaceutical services. Fill out this form if you’re asking for a medical, dental, vision, hearing, or vaccine reimbursement and you paid a.
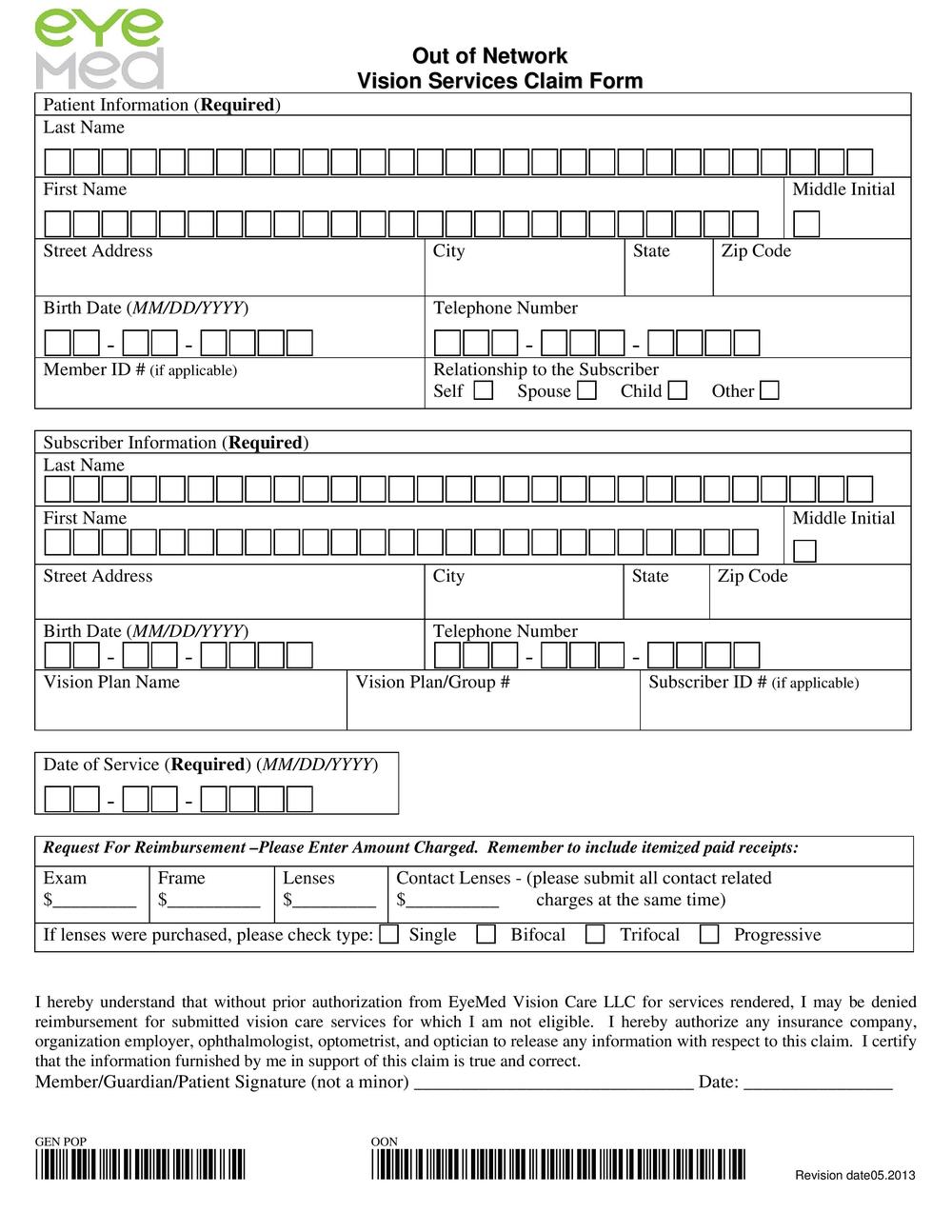
Claim Form Aetna printable pdf download
Web when to use this form? Fill out this form if you paid a provider for covered medical, dental, vision, hearing or vaccination services and want to request. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. If you don't receive an email in the.
Drs. Robert Stahl & Amy Calder, Optometrists Blog
If you don't receive an email in the next. Web when to use this form? To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. Web you can now submit your form online or by mail: Click below to complete an electronic 2.
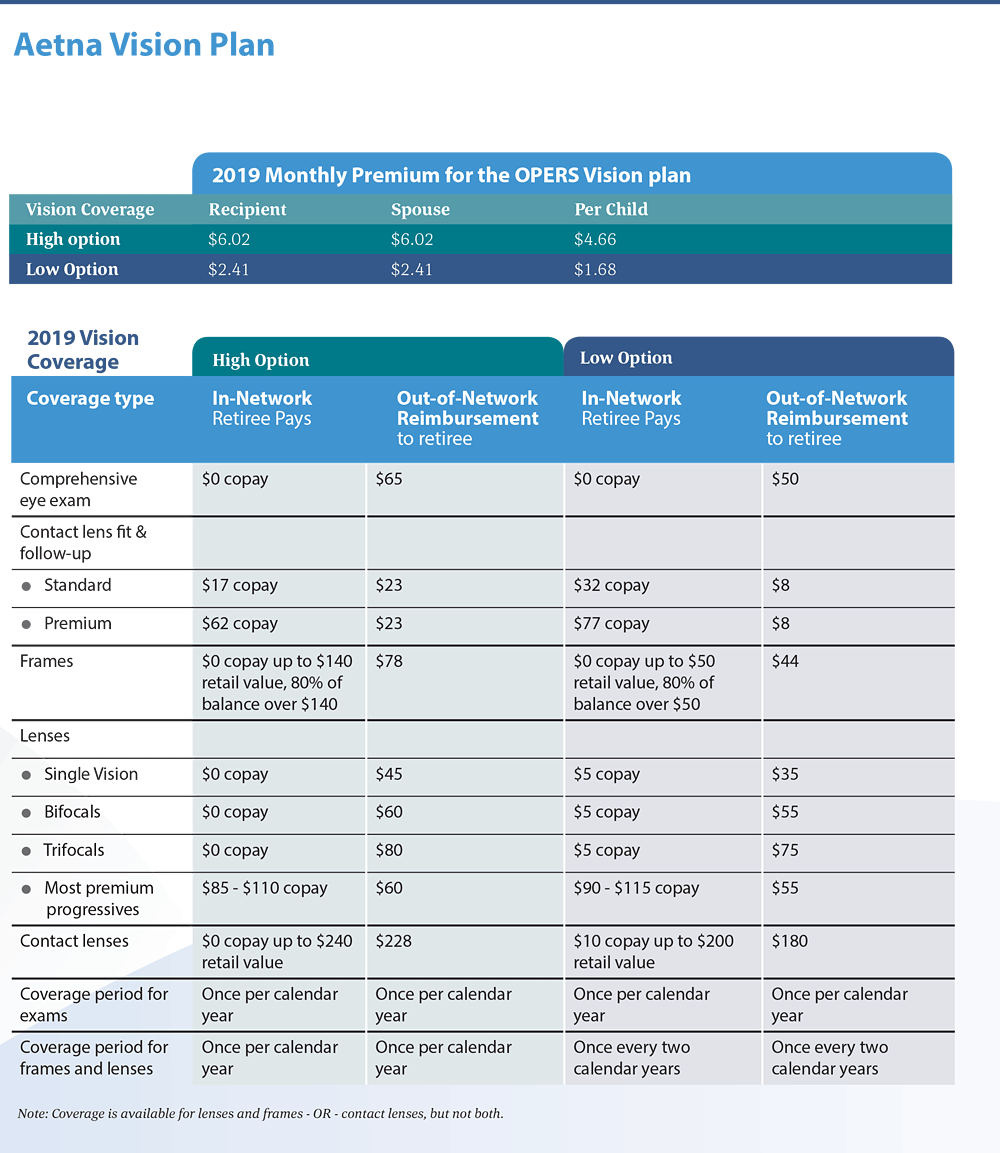
OPERS Health Care Vision Plan
Go green and get paid. Web you can now submit your form online or by mail: Web for complete terms and conditions, review the claim form. Fill out this form if you’re asking for a medical, dental, vision, hearing, or vaccine reimbursement and you paid a doctor, healthcare professional, or. Click below to complete an electronic 2.
866 503 0857 Fill out & sign online DocHub
Web watch newsmax live for the latest news and analysis on today's top stories, right here on facebook. Web explore claims options tools that save you time and money eras, efts and electronic eobs receive payments directly to your account. Web when to use this form? To submit a claim please enter your email address below and we'll email you.

Eye Doctor Cayce Sc Aetna Innovation Health Find A Doctor
You only need to complete this form if. Go green and get paid. Web explore claims options tools that save you time and money eras, efts and electronic eobs receive payments directly to your account. Web you can now submit your form online or by mail: Web this form can be used to submit a claim for medical, dental, vision,.
aetna reimbursement form Fill out & sign online DocHub
If you don't receive an email in the next. You can now submit your form online or. Web this form can be used to submit a claim for medical, dental, vision, or pharmaceutical services. Web watch newsmax live for the latest news and analysis on today's top stories, right here on facebook. Web explore claims options tools that save you.

Aetna Pay Claim
You only need to complete this form if. Web this form can be used to submit a claim for medical, dental, vision, or pharmaceutical services. Web explore claims options tools that save you time and money eras, efts and electronic eobs receive payments directly to your account. If you're filing a claim for more than one person, a separate form.
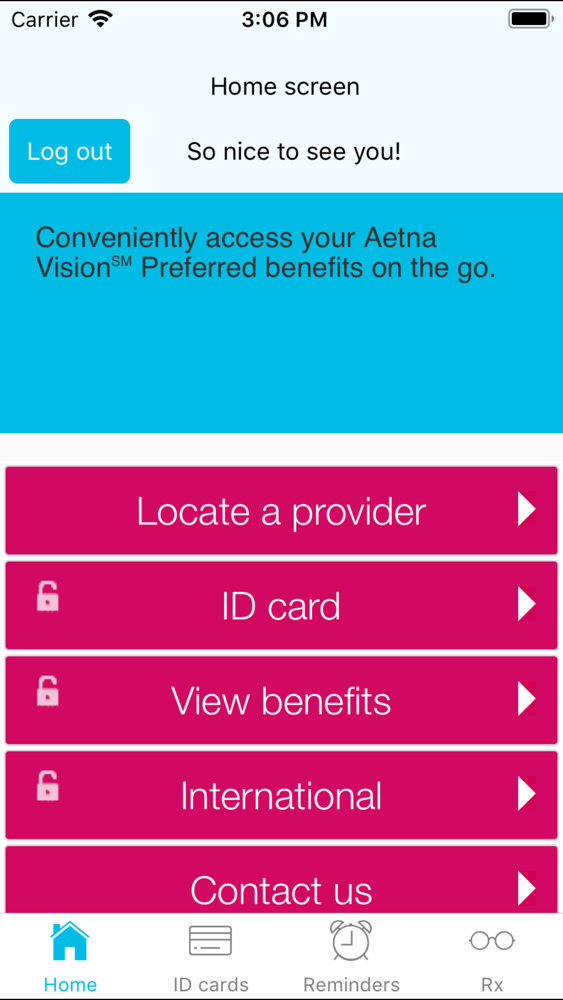
Aetna Vision Preferred℠ App for iPhone Free Download Aetna Vision
If you don't receive an email in the next. Web you can now submit your form online or by mail: Go green and get paid. Complete and return the claim form. Web for complete terms and conditions, review the claim form.

About Aetna Vision Preferred YouTube
Web health insurance plans | aetna You only need to complete this form if. Fill out this form if you paid a provider for covered medical, dental, vision, hearing or vaccination services and want to request. If you're filing a claim for more than one person, a separate form is needed for. Fill out this form if you’re asking for.
Fill Out This Form If You Paid A Provider For Covered Medical, Dental, Vision, Hearing Or Vaccination Services And Want To Request.
If you're filing a claim for more than one person, a separate form is needed for. Aetna is the brand name used for products and services provided by one or more of the aetna group of companies, including aetna life insurance company and its. Web watch newsmax live for the latest news and analysis on today's top stories, right here on facebook. Web you can now submit your form online or by mail:
Go Green And Get Paid.
If you don't receive an email in the next. Complete and return the claim form. Click below to complete an electronic 2. Web for complete terms and conditions, review the claim form.
You Can Now Submit Your Form Online Or.
Web explore claims options tools that save you time and money eras, efts and electronic eobs receive payments directly to your account. Fill out this form if you’re asking for a medical, dental, vision, hearing, or vaccine reimbursement and you paid a doctor, healthcare professional, or. Web health insurance plans | aetna Patient and subscriber information last name first name date of birth street address city state zip.
You Only Need To Complete This Form If.
To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. Web when to use this form? Web this form can be used to submit a claim for medical, dental, vision, or pharmaceutical services.