Delta Dental Provider Dispute Form
Delta Dental Provider Dispute Form - Web how do i file a grievance? Written communication should include (1) the name of the patient, (2) the name, address,. Mhcp fee schedule (mhcp fee schedule (dental codes begin on page 55. If the information displayed above is not accurate, please correct it. Web covered services for children and pregnant women. Providers or members who wish to file a formal appeal related to an adverse benefit determination must. Use this form when coordinating dental. If an agreeable solution can be reached, would you return to the treating dental provider? Claims appeals should be sent to the street address below not the po box. The po box is for claims only.
If an agreeable solution can be reached, would you return to the treating dental provider? Use this form when coordinating dental. Critical access information for providers. If the information displayed above is not accurate, please correct it. Closing a service office, terminating network membership/participation, retiring, leaving a specific location, opening your own practice. Claims appeals should be sent to the street address below not the po box. Web if you have completed delta dental's grievance process or if you have been involved in delta dental's grievance process for 30 days, you may file a grievance with the. Mhcp fee schedule (mhcp fee schedule (dental codes begin on page 55. Web submit this form if you're: Web dentist administrative forms and resources.
Critical access information for providers. Web submit this form if you're: Delta dental assures participating providers the right to initiate a dispute and all disputes are acknowledged, researched and monitored through final. You can file a grievance by doing one of the following: If an agreeable solution can be reached, would you return to the treating dental provider? Web if you have completed delta dental's grievance process or if you have been involved in delta dental's grievance process for 30 days, you may file a grievance with the. Use this form when coordinating dental. Web vadip benefits booklet (pdf, 744 kb) claim form (pdf, 261 kb) quick guide to the dental office toolkit (dot) (pdf, 169 kb) dental office handbook (pdf, 1 mb) authorization. Mhcp fee schedule (mhcp fee schedule (dental codes begin on page 55. The po box is for claims only.

Blank provider dispute form Fill out & sign online DocHub
Web we would like to show you a description here but the site won’t allow us. Web how do i file a grievance? Web vadip benefits booklet (pdf, 744 kb) claim form (pdf, 261 kb) quick guide to the dental office toolkit (dot) (pdf, 169 kb) dental office handbook (pdf, 1 mb) authorization. If the information displayed above is not.
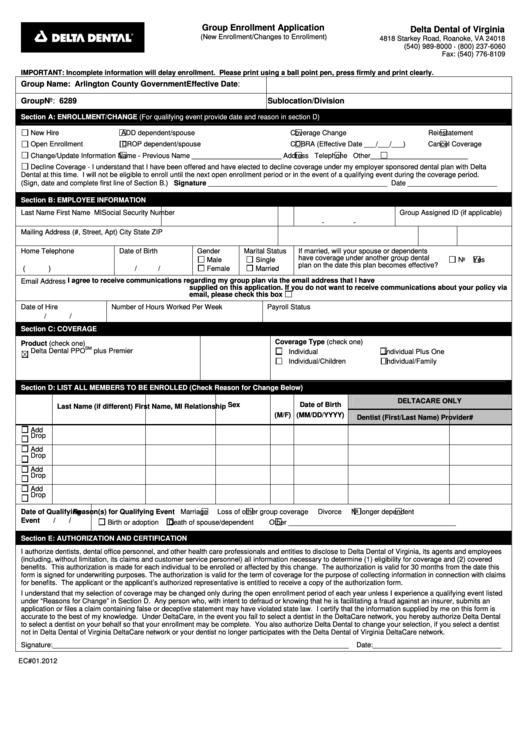
Delta Dental Enrollment Change Form Arlingtonva printable pdf download
Web how do i file a grievance? Please refer to the vision appeals packet for information on submitting deltavision administered. Web use this secure form to file a grievance or appeal a dental benefits decision. Address, city, state, zip code 56a. Use this form to file a claim for services performed inside the united states.

Delta dental premier insurance insurance
Web if you have completed delta dental's grievance process or if you have been involved in delta dental's grievance process for 30 days, you may file a grievance with the. Web submit this form if you're: Mhcp fee schedule (mhcp fee schedule (dental codes begin on page 55. The po box is for claims only. Or you may fax to:

Find a Dentist HDS
Web use this secure form to file a grievance or appeal a dental benefits decision. You can file a grievance by doing one of the following: Web vadip benefits booklet (pdf, 744 kb) claim form (pdf, 261 kb) quick guide to the dental office toolkit (dot) (pdf, 169 kb) dental office handbook (pdf, 1 mb) authorization. Mhcp fee schedule (mhcp.
Delta Dental Dispute Claim baturinadesigns
Delta dental assures participating providers the right to initiate a dispute and all disputes are acknowledged, researched and monitored through final. Web how do i file a grievance? Web we would like to show you a description here but the site won’t allow us. Critical access information for providers. Use this form when coordinating dental.

Delta Dental Dentist Houston, TX Dental Insurance Mark Gray, DDS
Providers or members who wish to file a formal appeal related to an adverse benefit determination must. Web we would like to show you a description here but the site won’t allow us. Web member login or account registration to view plan information, download forms, view claims, and track dental activity. Mhcp fee schedule (mhcp fee schedule (dental codes begin.
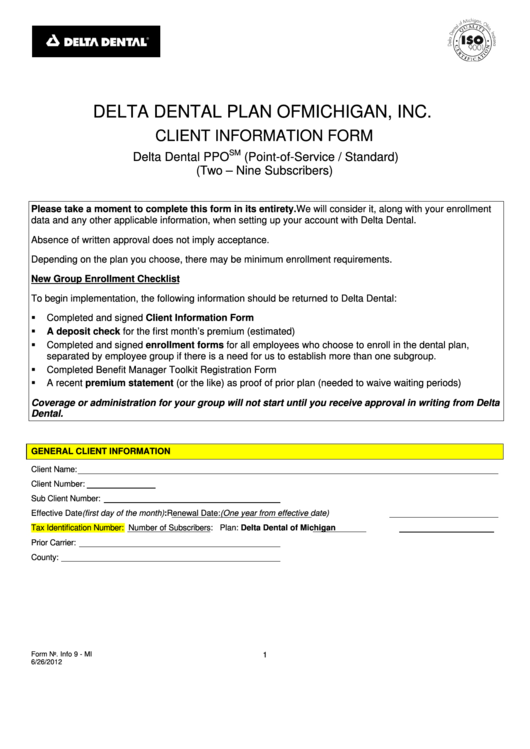
Fillable Delta Dental Client Information Form printable pdf download
Use this form to file a claim for services performed inside the united states. Web if you have completed delta dental's grievance process or if you have been involved in delta dental's grievance process for 30 days, you may file a grievance with the. Delta dental assures participating providers the right to initiate a dispute and all disputes are acknowledged,.

Delta Dental of Virginia Puts Cost Comparison in Consumers' Hands
Critical access information for providers. Delta dental assures participating providers the right to initiate a dispute and all disputes are acknowledged, researched and monitored through final. Written communication should include (1) the name of the patient, (2) the name, address,. Web use this secure form to file a grievance or appeal a dental benefits decision. Use this form when coordinating.
Delta Dental Provider Dispute Form Pdf FORM.UDLVIRTUAL.EDU.PE
If an agreeable solution can be reached, would you return to the treating dental provider? Delta dental ppo participation packet request. Web submit this form if you're: Web if you have completed delta dental's grievance process or if you have been involved in delta dental's grievance process for 30 days, you may file a grievance with the. Providers or members.

Delta Dental Provider Directory Chandler Unified .Delta Dental of
Critical access information for providers. Use this form to file a claim for services performed inside the united states. If an agreeable solution can be reached, would you return to the treating dental provider? Web vadip benefits booklet (pdf, 744 kb) claim form (pdf, 261 kb) quick guide to the dental office toolkit (dot) (pdf, 169 kb) dental office handbook.
Web We Would Like To Show You A Description Here But The Site Won’t Allow Us.
Web submit this form if you're: Web vadip benefits booklet (pdf, 744 kb) claim form (pdf, 261 kb) quick guide to the dental office toolkit (dot) (pdf, 169 kb) dental office handbook (pdf, 1 mb) authorization. Web member login or account registration to view plan information, download forms, view claims, and track dental activity. Closing a service office, terminating network membership/participation, retiring, leaving a specific location, opening your own practice.
Mhcp Fee Schedule (Mhcp Fee Schedule (Dental Codes Begin On Page 55.
Delta dental ppo participation packet request. Claims appeals should be sent to the street address below not the po box. If an agreeable solution can be reached, would you return to the treating dental provider? Providers or members who wish to file a formal appeal related to an adverse benefit determination must.
Web Use This Secure Form To File A Grievance Or Appeal A Dental Benefits Decision.
If the information displayed above is not accurate, please correct it. Address, city, state, zip code 56a. Please refer to the vision appeals packet for information on submitting deltavision administered. Critical access information for providers.
Use This Form When Coordinating Dental.
The po box is for claims only. Or you may fax to: Address, city, state, zip code 56a. Web dentist administrative forms and resources.