Dwc Form 005
Dwc Form 005 - Web division of workers' compensation subject: Steps to electronically submit a form to the division of workers’ compensation: Any other topic related to the department of industrial. It explains the rights and responsibilities of both employers and employees under the law. Forms are grouped by relevant subject, then in alphabetical order. Google chrome and microsoft edge. Use the arrows to change to reverse alphabetical order or search by form number. Employers must post this form at each workplace and provide. Do not have workers' compensation insurance, or you have terminated your. You terminated workers' compensation insurance coverage, then the start date is the first date you did not have coverage.
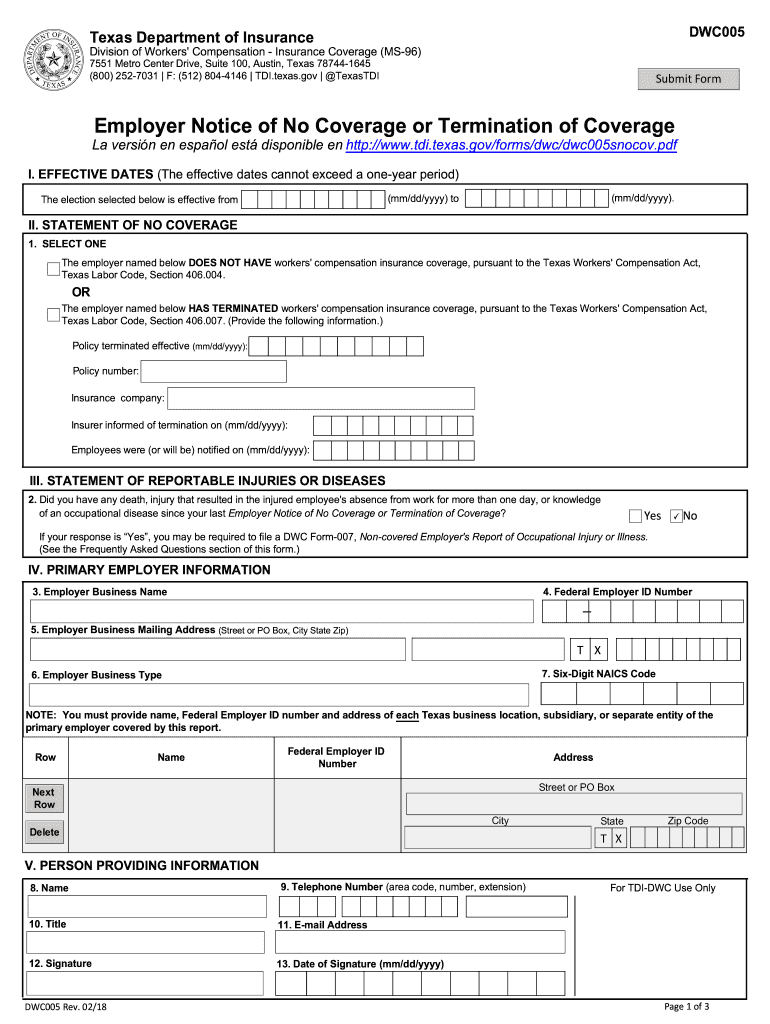
Do not have workers' compensation insurance, or you have terminated your. Forms are grouped by relevant subject, then in alphabetical order. Google chrome and microsoft edge. Web division of workers' compensation subject: You terminated workers' compensation insurance coverage, then the start date is the first date you did not have coverage. Use the arrows to change to reverse alphabetical order or search by form number. Web statement of no coverage or termination of coverage for employeesthis form is for employers who do not have or have ended their workers' compensation insurance coverage in texas. Any other topic related to the department of industrial. Employers must post this form at each workplace and provide. Web dwc005 , employer notice of no coverage or termination of coverage.
It explains the rights and responsibilities of both employers and employees under the law. Web division of workers' compensation subject: Google chrome and microsoft edge. Web dwc005 , employer notice of no coverage or termination of coverage. You terminated workers' compensation insurance coverage, then the start date is the first date you did not have coverage. Web statement of no coverage or termination of coverage for employeesthis form is for employers who do not have or have ended their workers' compensation insurance coverage in texas. Any other topic related to the department of industrial. Check out our video tutorial below for help filling out this form. Employers must post this form at each workplace and provide. Forms are grouped by relevant subject, then in alphabetical order.
Dwc005 Fill Out and Sign Printable PDF Template signNow
Employers must post this form at each workplace and provide. Web statement of no coverage or termination of coverage for employeesthis form is for employers who do not have or have ended their workers' compensation insurance coverage in texas. Do not have workers' compensation insurance, or you have terminated your. Web division of workers' compensation subject: Use the arrows to.
TX DWC Form 82 2005 Fill and Sign Printable Template Online US
Web statement of no coverage or termination of coverage for employeesthis form is for employers who do not have or have ended their workers' compensation insurance coverage in texas. Do not have workers' compensation insurance, or you have terminated your. Check out our video tutorial below for help filling out this form. You terminated workers' compensation insurance coverage, then the.

DWC 1 Form Fill out Online Template in PDF
Do not have workers' compensation insurance, or you have terminated your. Web division of workers' compensation subject: Google chrome and microsoft edge. Check out our video tutorial below for help filling out this form. You terminated workers' compensation insurance coverage, then the start date is the first date you did not have coverage.

Wage Statement Online Fill Online, Printable, Fillable, Blank pdfFiller
Forms are grouped by relevant subject, then in alphabetical order. Check out our video tutorial below for help filling out this form. Do not have workers' compensation insurance, or you have terminated your. Steps to electronically submit a form to the division of workers’ compensation: You terminated workers' compensation insurance coverage, then the start date is the first date you.
Fillable Dwc Form153 Request For Copies Of Confidential Claimant
Employers must post this form at each workplace and provide. Use the arrows to change to reverse alphabetical order or search by form number. Check out our video tutorial below for help filling out this form. Google chrome and microsoft edge. Steps to electronically submit a form to the division of workers’ compensation:
Form DWC1S Download Fillable PDF or Fill Online Employers First Report
Forms are grouped by relevant subject, then in alphabetical order. Web division of workers' compensation subject: Any other topic related to the department of industrial. Steps to electronically submit a form to the division of workers’ compensation: Use the arrows to change to reverse alphabetical order or search by form number.
2010 CA DWC Form 10232.2 Fill Online, Printable, Fillable, Blank
Employers must post this form at each workplace and provide. Forms are grouped by relevant subject, then in alphabetical order. Check out our video tutorial below for help filling out this form. Google chrome and microsoft edge. Use the arrows to change to reverse alphabetical order or search by form number.

Dwc 25 Fillable Form Pdf Fill and Sign Printable Template Online US
You terminated workers' compensation insurance coverage, then the start date is the first date you did not have coverage. Employers must post this form at each workplace and provide. Forms are grouped by relevant subject, then in alphabetical order. Steps to electronically submit a form to the division of workers’ compensation: Any other topic related to the department of industrial.
DWC Form 9767.16.5 Download Fillable PDF or Fill Online DWC Medical
Do not have workers' compensation insurance, or you have terminated your. Steps to electronically submit a form to the division of workers’ compensation: Any other topic related to the department of industrial. It explains the rights and responsibilities of both employers and employees under the law. Employers must post this form at each workplace and provide.

Dwc 102531 Form Pdf Fill Online, Printable, Fillable, Blank PDFfiller
Google chrome and microsoft edge. Employers must post this form at each workplace and provide. Web dwc005 , employer notice of no coverage or termination of coverage. Do not have workers' compensation insurance, or you have terminated your. You terminated workers' compensation insurance coverage, then the start date is the first date you did not have coverage.
Use The Arrows To Change To Reverse Alphabetical Order Or Search By Form Number.
Check out our video tutorial below for help filling out this form. It explains the rights and responsibilities of both employers and employees under the law. Steps to electronically submit a form to the division of workers’ compensation: Web statement of no coverage or termination of coverage for employeesthis form is for employers who do not have or have ended their workers' compensation insurance coverage in texas.
Employers Must Post This Form At Each Workplace And Provide.
Any other topic related to the department of industrial. Forms are grouped by relevant subject, then in alphabetical order. You terminated workers' compensation insurance coverage, then the start date is the first date you did not have coverage. Do not have workers' compensation insurance, or you have terminated your.
Google Chrome And Microsoft Edge.
Web division of workers' compensation subject: Web dwc005 , employer notice of no coverage or termination of coverage.