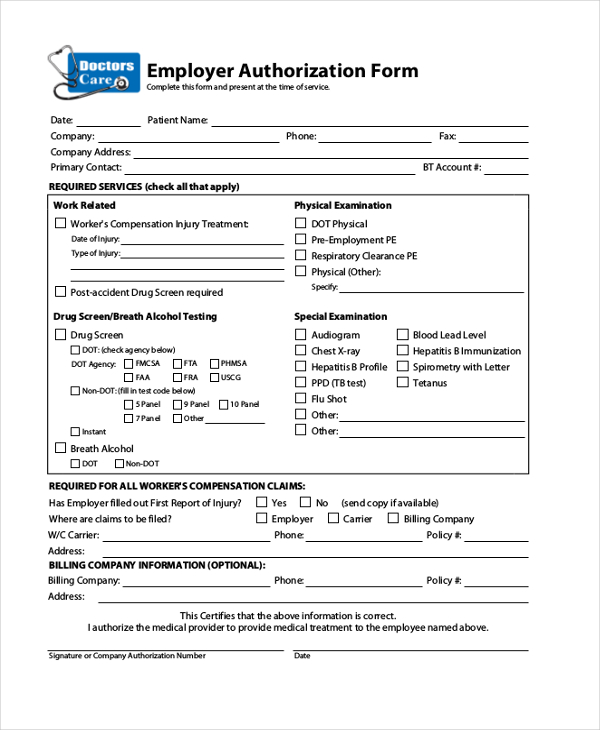
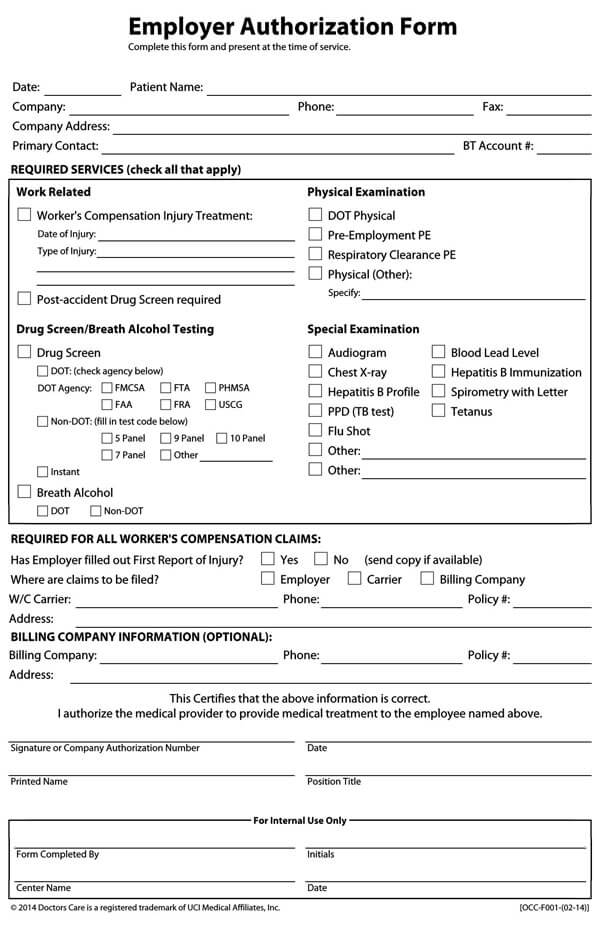
Employer Authorization Form
Employer Authorization Form - You will need to apply for an ead if you: _____ work related physical examination t injury t illness t preplacement t baseline t annual t exit date of injury_____ dot physical examination breath alcohol special examination substance abuse testing It is important that you write the correct eligibility category on your application. Preventing discrimination we provide information on employee rights and preventing discrimination in the workplace. Web employer:_____ date of birth: This includes citizens and noncitizens. Employer information der/company contact for results and/or physician call: Web employer authorization form name and title (please print) signature:
Web employer:_____ date of birth: It is important that you write the correct eligibility category on your application. You will need to apply for an ead if you: _____ work related physical examination t injury t illness t preplacement t baseline t annual t exit date of injury_____ dot physical examination breath alcohol special examination substance abuse testing Preventing discrimination we provide information on employee rights and preventing discrimination in the workplace. This includes citizens and noncitizens. Web employer authorization form name and title (please print) signature: Employer information der/company contact for results and/or physician call:
You will need to apply for an ead if you: Web employer:_____ date of birth: Preventing discrimination we provide information on employee rights and preventing discrimination in the workplace. _____ work related physical examination t injury t illness t preplacement t baseline t annual t exit date of injury_____ dot physical examination breath alcohol special examination substance abuse testing It is important that you write the correct eligibility category on your application. This includes citizens and noncitizens. Employer information der/company contact for results and/or physician call: Web employer authorization form name and title (please print) signature:

Wellmed Prior Authorization Form Fill Online, Printable, Fillable
It is important that you write the correct eligibility category on your application. Employer information der/company contact for results and/or physician call: Web employer:_____ date of birth: Web employer authorization form name and title (please print) signature: You will need to apply for an ead if you:
FREE 5+ Employment Authorization Forms in PDF
Web employer authorization form name and title (please print) signature: It is important that you write the correct eligibility category on your application. Preventing discrimination we provide information on employee rights and preventing discrimination in the workplace. This includes citizens and noncitizens. Employer information der/company contact for results and/or physician call:
Authorization To Allow Employment Verification / Form I 9 Wikipedia
Employer information der/company contact for results and/or physician call: Preventing discrimination we provide information on employee rights and preventing discrimination in the workplace. Web employer:_____ date of birth: This includes citizens and noncitizens. You will need to apply for an ead if you:
FREE 10+ Sample Direct Deposit Authorization Forms in PDF MS Word
Web employer:_____ date of birth: This includes citizens and noncitizens. _____ work related physical examination t injury t illness t preplacement t baseline t annual t exit date of injury_____ dot physical examination breath alcohol special examination substance abuse testing Web employer authorization form name and title (please print) signature: Preventing discrimination we provide information on employee rights and preventing.
FREE 10+ Sample Medical Authorization Forms in PDF MS Word Excel
You will need to apply for an ead if you: Web employer:_____ date of birth: This includes citizens and noncitizens. Web employer authorization form name and title (please print) signature: Employer information der/company contact for results and/or physician call:
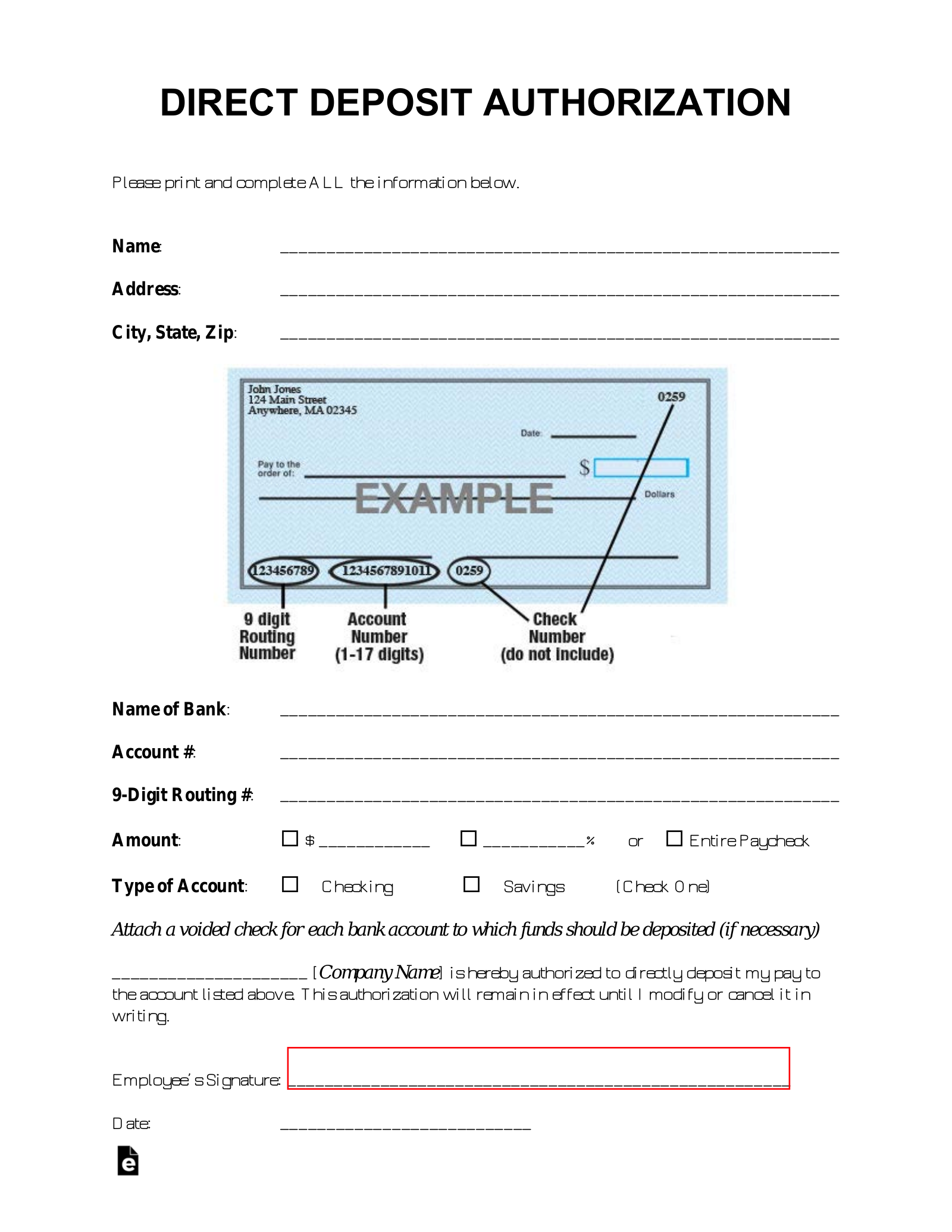
Free Direct Deposit Authorization Forms (22) PDF Word eForms
Web employer authorization form name and title (please print) signature: You will need to apply for an ead if you: Employer information der/company contact for results and/or physician call: Preventing discrimination we provide information on employee rights and preventing discrimination in the workplace. This includes citizens and noncitizens.
Free Medical Authorization Forms & Templates (Word PDF)
Preventing discrimination we provide information on employee rights and preventing discrimination in the workplace. Employer information der/company contact for results and/or physician call: You will need to apply for an ead if you: _____ work related physical examination t injury t illness t preplacement t baseline t annual t exit date of injury_____ dot physical examination breath alcohol special examination.

Example Of Employment Authorization Form Sample Templates
This includes citizens and noncitizens. Web employer authorization form name and title (please print) signature: Preventing discrimination we provide information on employee rights and preventing discrimination in the workplace. Web employer:_____ date of birth: _____ work related physical examination t injury t illness t preplacement t baseline t annual t exit date of injury_____ dot physical examination breath alcohol special.
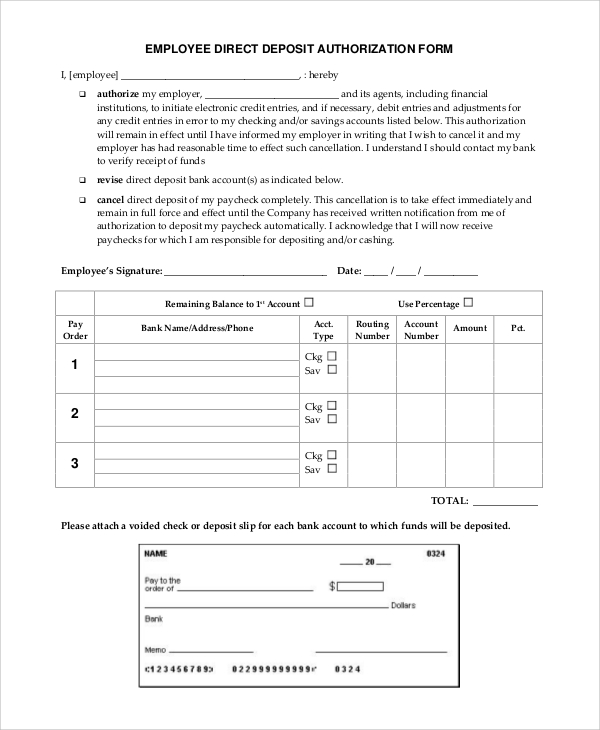
FREE 10+ Sample Direct Deposit Authorization Forms in PDF MS Word
Web employer authorization form name and title (please print) signature: You will need to apply for an ead if you: Employer information der/company contact for results and/or physician call: Web employer:_____ date of birth: Preventing discrimination we provide information on employee rights and preventing discrimination in the workplace.

Third Party Authorization Form Sample and Template
This includes citizens and noncitizens. Web employer authorization form name and title (please print) signature: Employer information der/company contact for results and/or physician call: It is important that you write the correct eligibility category on your application. Preventing discrimination we provide information on employee rights and preventing discrimination in the workplace.
Web Employer Authorization Form Name And Title (Please Print) Signature:
Preventing discrimination we provide information on employee rights and preventing discrimination in the workplace. Web employer:_____ date of birth: This includes citizens and noncitizens. It is important that you write the correct eligibility category on your application.
_____ Work Related Physical Examination T Injury T Illness T Preplacement T Baseline T Annual T Exit Date Of Injury_____ Dot Physical Examination Breath Alcohol Special Examination Substance Abuse Testing
Employer information der/company contact for results and/or physician call: You will need to apply for an ead if you: