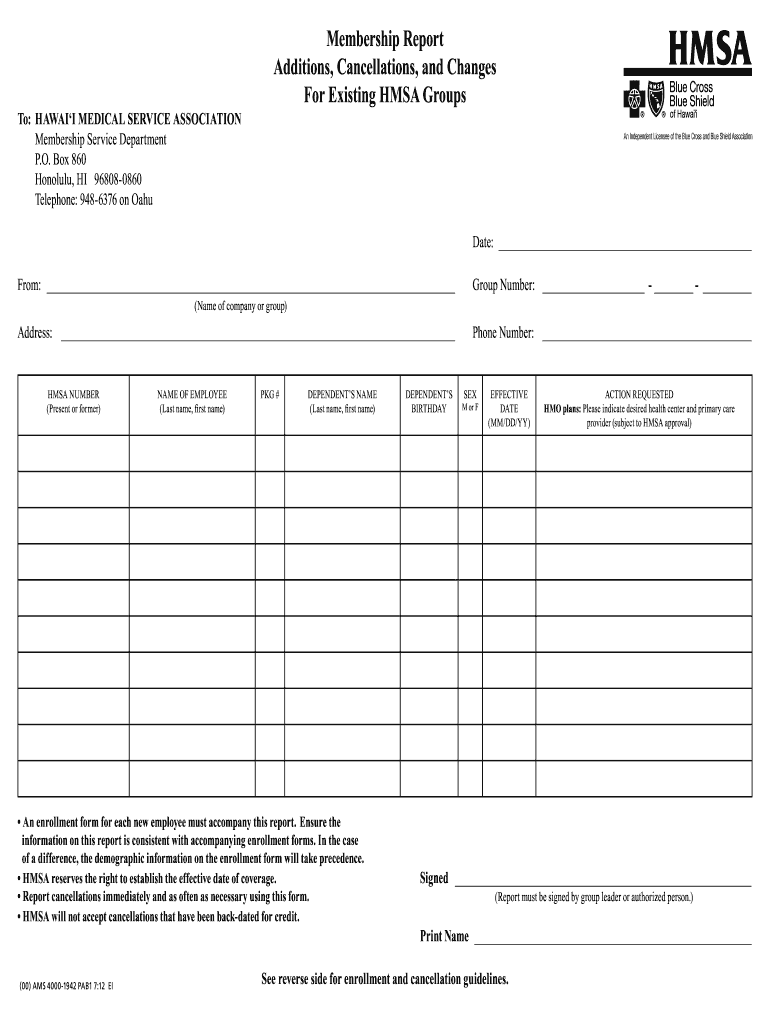
Hmsa Enrollment Form
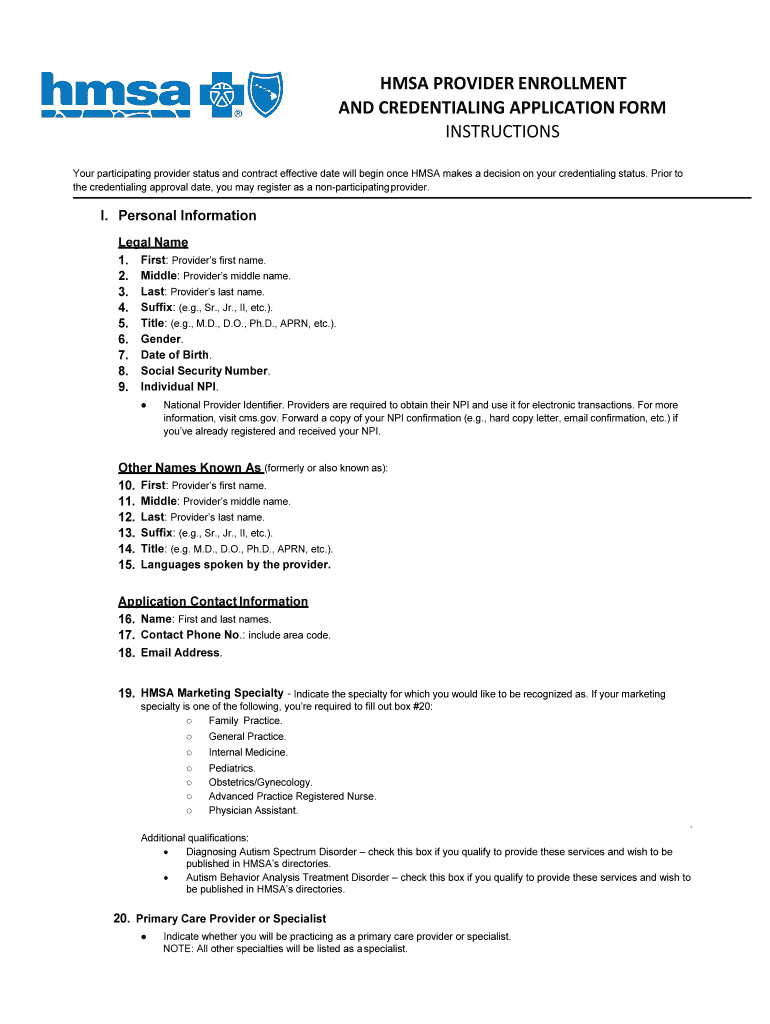
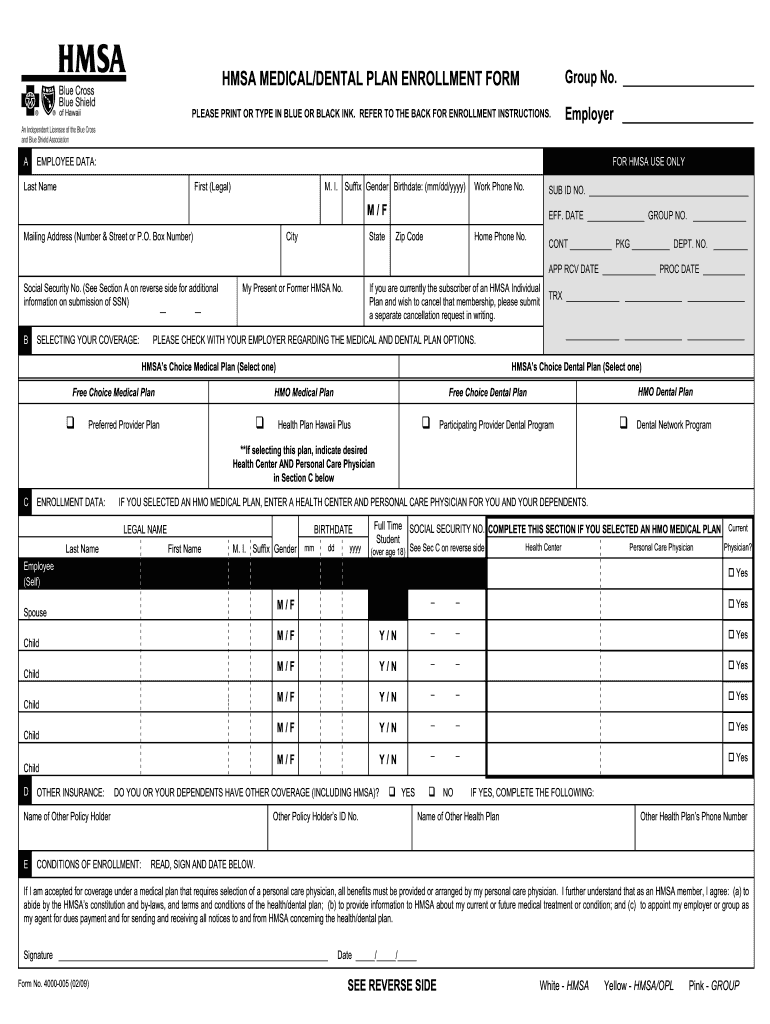
Hmsa Enrollment Form - Web send hmsa provider enrollment forms via email, link, or fax. Need help using the application? This coverage takes effect and your employees are eligible to receive benefits on their plan’s effective date as long as: Web complete hmsa provider enrollment and credentialing application form instructions for individual provider online with us legal forms. Web how do i get help with this form? • electronic trading partner agreement where should i send the form(s)? Web how do i get help with this form? You can also download it, export it or print it out. Read, sign and date below. Employee data select the enrollment type for which you are submitting the enrol lment form.
• electronic trading partner agreement where should i send the form(s)? If i am accepted for coverage under a medical plan that requires selection of a primary care provider, all benefits must be. Web hmsa, an independent licensee of the blue cross and blue shield association. You can also download it, export it or print it out. This coverage takes effect and your employees are eligible to receive benefits on their plan’s effective date as long as: The easiest way to edit hmsa medical form in pdf format online Or call medicare at 1 (800). Read, sign and date below. Electronic funds transfer (eft) authorization agreement submission information provider tax identification number (tin) national provider identifier (npi) reason for. Web send hmsa provider enrollment forms via email, link, or fax.
Web hmsa, an independent licensee of the blue cross and blue shield association. Or call medicare at 1 (800). Web how do i get help with this form? • electronic trading partner agreement where should i send the form(s)? Tty users can call 711. Hmsa authorized representative form(optional) the enclosed authorized representative form is used tell us which family members or friends you authorize us to. If i am accepted for coverage under a medical plan that requires selection of a primary care provider, all benefits must be. Electronic funds transfer (eft) authorization agreement submission information provider tax identification number (tin) national provider identifier (npi) reason for. Request for taxpayer identification number and certification or copy of irs letter 147c copy of general liability insurance certificate the coverage amount we. Easily fill out pdf blank, edit, and sign.

(PDF) HMSA Provider Enrollment and Credentialing Application · 201909
Tty users can call 711. Or call medicare at 1. Or call medicare at 1 (800). Need help using the application? Electronic funds transfer (eft) authorization agreement submission information provider tax identification number (tin) national provider identifier (npi) reason for.

Maui County Financial Data More Accessible Through Web Portal Maui Now
Web hmsa, an independent licensee of the blue cross and blue shield association. Request for taxpayer identification number and certification or copy of irs letter 147c copy of general liability insurance certificate the coverage amount we. Web hmsa enrollment form 2020. Read, sign and date below. Need help using the application?
Hmsa Online Care Provider Enrollment Form Enrollment Form
Web what form(s) should i do? You can also download it, export it or print it out. The easiest way to edit hmsa medical form in pdf format online Web complete hmsa provider enrollment and credentialing application form instructions for individual provider online with us legal forms. Hr registration benefit enrollment login login id forgot.

HMSA Foundation Supports Efforts to Develop Healthcare Workforce on
Electronic funds transfer (eft) authorization agreement submission information provider tax identification number (tin) national provider identifier (npi) reason for. Mark the new hire box if you’re newly hired,. Hmsa authorized representative form(optional) the enclosed authorized representative form is used tell us which family members or friends you authorize us to. Web what form(s) should i do? • electronic trading partner.
Hmsa Enroll Fill Out and Sign Printable PDF Template signNow
You can also download it, export it or print it out. Web hmsa, an independent licensee of the blue cross and blue shield association. Read, sign and date below. If i am accepted for coverage under a medical plan that requires selection of a primary care provider, all benefits must be. • mail original form to:
Hmsa Form Fill Out and Sign Printable PDF Template signNow
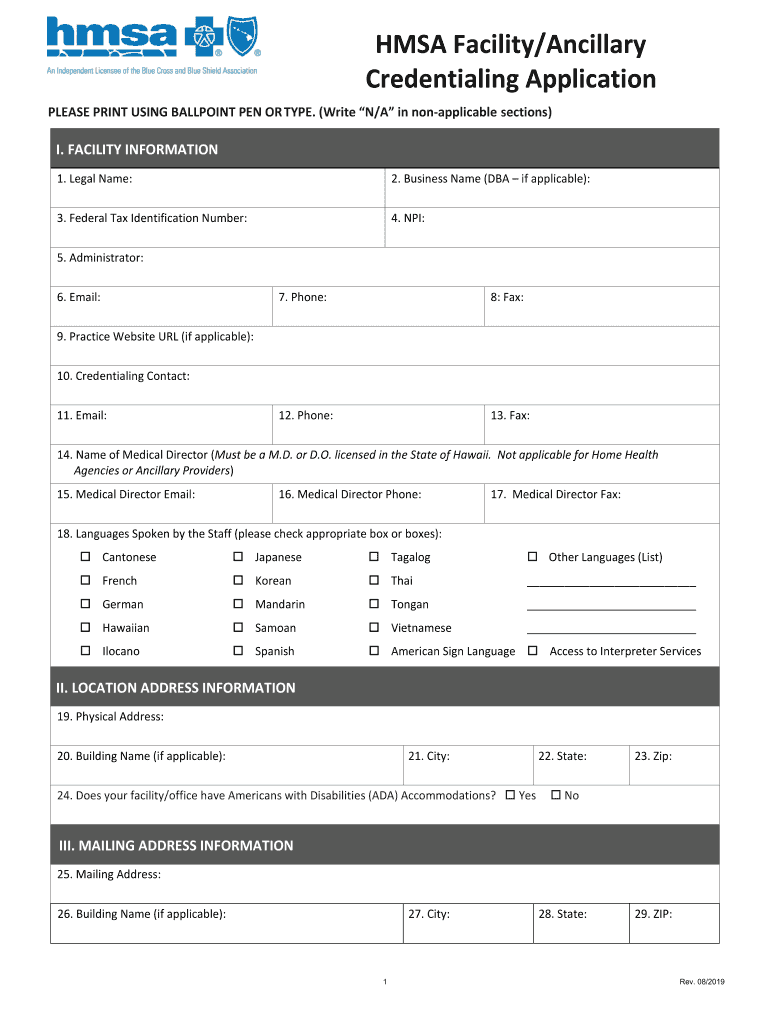
Hmsa authorized representative form(optional) the enclosed authorized representative form is used tell us which family members or friends you authorize us to. Web how do i get help with this form? • electronic trading partner agreement where should i send the form(s)? Provider application form for business/facility. Hr registration benefit enrollment login login id forgot.
Hmsa Credentialing Fill Out and Sign Printable PDF Template signNow
Mark the new hire box if you’re newly hired,. Web send hmsa provider enrollment forms via email, link, or fax. • mail original form to: • electronic trading partner agreement where should i send the form(s)? The easiest way to edit hmsa medical form in pdf format online
Hawaii EmployerUnion Health Benefits Trust Fund HMSA Subcontractors
Web what form(s) should i do? Request for taxpayer identification number and certification or copy of irs letter 147c copy of general liability insurance certificate the coverage amount we. • mail original form to: You can also download it, export it or print it out. Mark the new hire box if you’re newly hired,.
Hmsa Cancellation Form Fill Online, Printable, Fillable, Blank
Web complete hmsa provider enrollment and credentialing application form instructions for individual provider online with us legal forms. Mark the new hire box if you’re newly hired,. Electronic funds transfer (eft) authorization agreement submission information provider tax identification number (tin) national provider identifier (npi) reason for. This coverage takes effect and your employees are eligible to receive benefits on their.

Hmsa Hmo Referral Form 20202021 Fill and Sign Printable Template
This coverage takes effect and your employees are eligible to receive benefits on their plan’s effective date as long as: Hmsa akamai advantage is a ppo plan with a medicare contract. Web hmsa enrollment form 2020. Easily fill out pdf blank, edit, and sign. If i am accepted for coverage under a medical plan that requires selection of a primary.
Web How Do I Get Help With This Form?
Web send hmsa provider enrollment forms via email, link, or fax. You can also download it, export it or print it out. Or call medicare at 1 (800). • electronic trading partner agreement where should i send the form(s)?
Hr Registration Benefit Enrollment Login Login Id Forgot.
Read, sign and date below. Web how do i get help with this form? Web complete hmsa provider enrollment and credentialing application form instructions for individual provider online with us legal forms. Web hmsa enrollment form 2020.
If I Am Accepted For Coverage Under A Medical Plan That Requires Selection Of A Primary Care Provider, All Benefits Must Be.
Employee data select the enrollment type for which you are submitting the enrol lment form. Hmsa akamai advantage is a ppo plan with a medicare contract. Easily fill out pdf blank, edit, and sign. Provider application form for business/facility.
Electronic Funds Transfer (Eft) Authorization Agreement Submission Information Provider Tax Identification Number (Tin) National Provider Identifier (Npi) Reason For.
Need help using the application? Or call medicare at 1. Request for taxpayer identification number and certification or copy of irs letter 147c copy of general liability insurance certificate the coverage amount we. • mail original form to: