Medicare Claim Appeal Form
Medicare Claim Appeal Form - Select the sample you need in our collection of legal forms. How to avoid duplicate claim denials. Web if an enrollee would like to appoint a person to file a grievance, request a coverage determination, or request an appeal on his or her behalf, the enrollee and the person. Web check your claim status with your secure medicare account, your medicare summary notice (msn), your explanation of benefits (eob), medicare's blue button, or contact. Web medicare reconsideration request form — 2nd level of appeal. If you want help filing an appeal,. Web this form usually comes from your healthcare provider and lets you know that you — not medicare — are responsible for paying for a service or equipment. There are 2 ways that a party can request a redetermination: Your next level of appeal is a reconsideration by a. Web get medicare forms for different situations, like filing a claim or appealing a coverage decision.
How to avoid duplicate claim denials. If you still disagree with the claim decision as an original medicare beneficiary, you have 120 days after receiving the msn to file an. Select the sample you need in our collection of legal forms. Web a redetermination must be requested in writing. Stick to these simple instructions to get medicare appeal form prepared for sending: If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Web get medicare forms for different situations, like filing a claim or appealing a coverage decision. Web this form usually comes from your healthcare provider and lets you know that you — not medicare — are responsible for paying for a service or equipment. Web medicare redetermination request form — 1st level of appeal beneficiary’s name (first, middle, last) if you received your initial determination notice. (portal) and register for an account.
Select your state to find out if you can file an appeal with the marketplace. Your next level of appeal is a reconsideration by a. Can someone file an appeal for me? Web get medicare forms for different situations, like filing a claim or appealing a coverage decision. Find forms publications read, print, or order free medicare publications in a. Stick to these simple instructions to get medicare appeal form prepared for sending: Beneficiary’s name (first, middle, last) medicare number. The form must be placed on top of all supporting information you provide. Select the sample you need in our collection of legal forms. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal.

Medicare Appeal Form Cms20027 Medicare (United States) Medicaid
Select your state to find out if you can file an appeal with the marketplace. How to avoid duplicate claim denials. Web if an enrollee would like to appoint a person to file a grievance, request a coverage determination, or request an appeal on his or her behalf, the enrollee and the person. Submit one form for each claim you.
Indiana Medicaid Appeal Form Fill Online, Printable, Fillable, Blank
Select the sample you need in our collection of legal forms. Web medicare reconsideration request form — 2nd level of appeal. Select your state to find out if you can file an appeal with the marketplace. Beneficiary’s name (first, middle, last) medicare number. Web get medicare forms for different situations, like filing a claim or appealing a coverage decision.
FREE 8+ Sample Medicare Forms in MS Word PDF
The form must be placed on top of all supporting information you provide. Then, click “next” to get forms or file your appeal online. Select your state to find out if you can file an appeal with the marketplace. Web if an enrollee would like to appoint a person to file a grievance, request a coverage determination, or request an.
FREE 40+ Claim Forms in PDF Excel MS Word
Web this form usually comes from your healthcare provider and lets you know that you — not medicare — are responsible for paying for a service or equipment. Web medicare redetermination request form — 1st level of appeal beneficiary’s name (first, middle, last) if you received your initial determination notice. Web get medicare forms for different situations, like filing a.

Cigna Appeal Request Fill and Sign Printable Template Online US
Web this form usually comes from your healthcare provider and lets you know that you — not medicare — are responsible for paying for a service or equipment. Stick to these simple instructions to get medicare appeal form prepared for sending: Web how do i file an appeal for my claim? (portal) and register for an account. Then, click “next”.

Was Your Medicare Claim Rejected? Here’s How to Appeal diaTribe
Can someone file an appeal for me? Web if an enrollee would like to appoint a person to file a grievance, request a coverage determination, or request an appeal on his or her behalf, the enrollee and the person. Find forms publications read, print, or order free medicare publications in a. Web it only takes a couple of minutes. Select.
Top United Healthcare Appeal Form Templates free to download in PDF format
Web get medicare forms for different situations, like filing a claim or appealing a coverage decision. If you want help filing an appeal,. Select the sample you need in our collection of legal forms. Can someone file an appeal for me? Submit one form for each claim you wish to appeal.
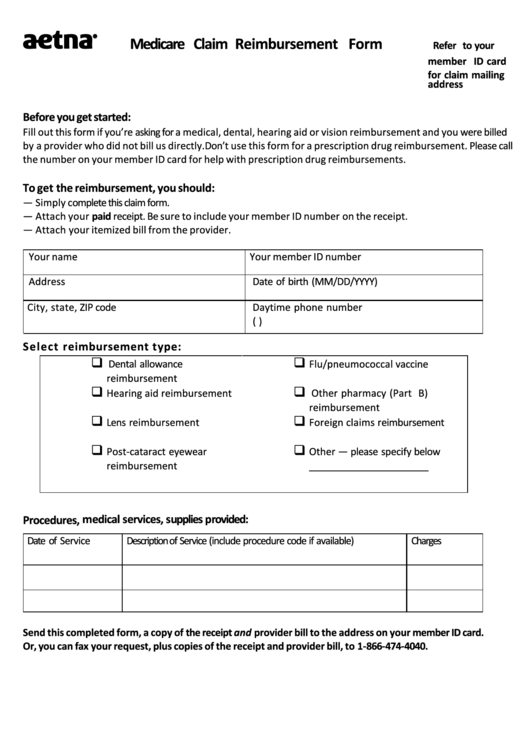
Top 84 Aetna Forms And Templates free to download in PDF format
There are 2 ways that a party can request a redetermination: Can someone file an appeal for me? Web medicare redetermination request form — 1st level of appeal beneficiary’s name (first, middle, last) if you received your initial determination notice. Stick to these simple instructions to get medicare appeal form prepared for sending: Web get medicare forms for different situations,.

Medicare Lift Chair Form Form Resume Examples Mj1v4Lk3wy
There are 2 ways that a party can request a redetermination: Date the service or item was. Web check your claim status with your secure medicare account, your medicare summary notice (msn), your explanation of benefits (eob), medicare's blue button, or contact. If you still disagree with the claim decision as an original medicare beneficiary, you have 120 days after.
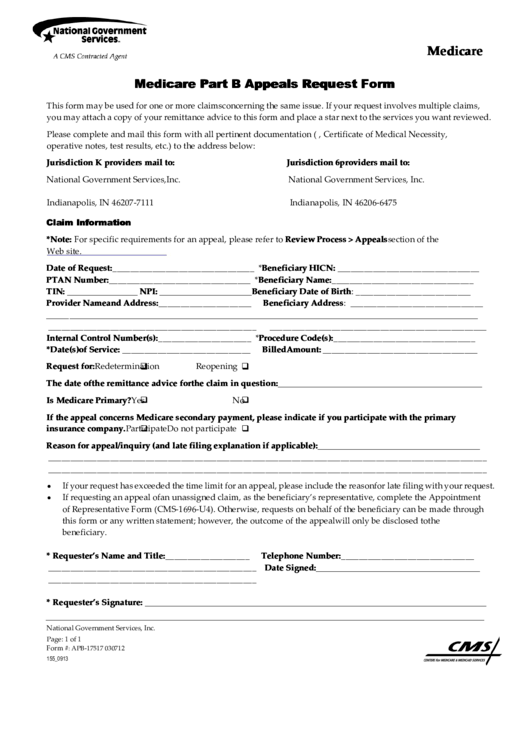
Medicare Part B Appeals Request Form printable pdf download
Date the service or item was. Web it only takes a couple of minutes. Then, click “next” to get forms or file your appeal online. Web a redetermination must be requested in writing. Submit one form for each claim you wish to appeal.
Web Medicare Redetermination Request Form — 1St Level Of Appeal Beneficiary’s Name (First, Middle, Last) If You Received Your Initial Determination Notice.
The form must be placed on top of all supporting information you provide. Beneficiary’s name (first, middle, last) medicare number. If you want help filing an appeal,. Web a redetermination must be requested in writing.
Web Get Medicare Forms For Different Situations, Like Filing A Claim Or Appealing A Coverage Decision.
Can someone file an appeal for me? Select your state to find out if you can file an appeal with the marketplace. Stick to these simple instructions to get medicare appeal form prepared for sending: Web how do i file an appeal for my claim?
There Are 2 Ways That A Party Can Request A Redetermination:
If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. If you still disagree with the claim decision as an original medicare beneficiary, you have 120 days after receiving the msn to file an. (portal) and register for an account. How to avoid duplicate claim denials.
Submit One Form For Each Claim You Wish To Appeal.
Web medicare reconsideration request form — 2nd level of appeal. Then, click “next” to get forms or file your appeal online. Web if an enrollee would like to appoint a person to file a grievance, request a coverage determination, or request an appeal on his or her behalf, the enrollee and the person. Date the service or item was.