Medicare Form L564
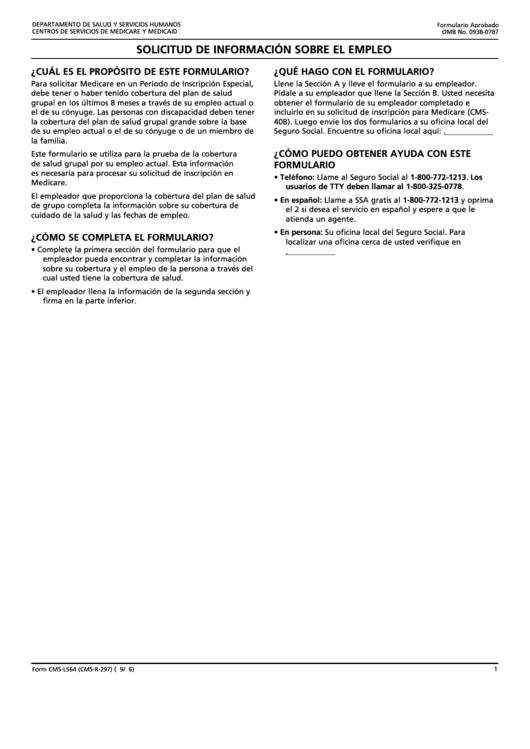
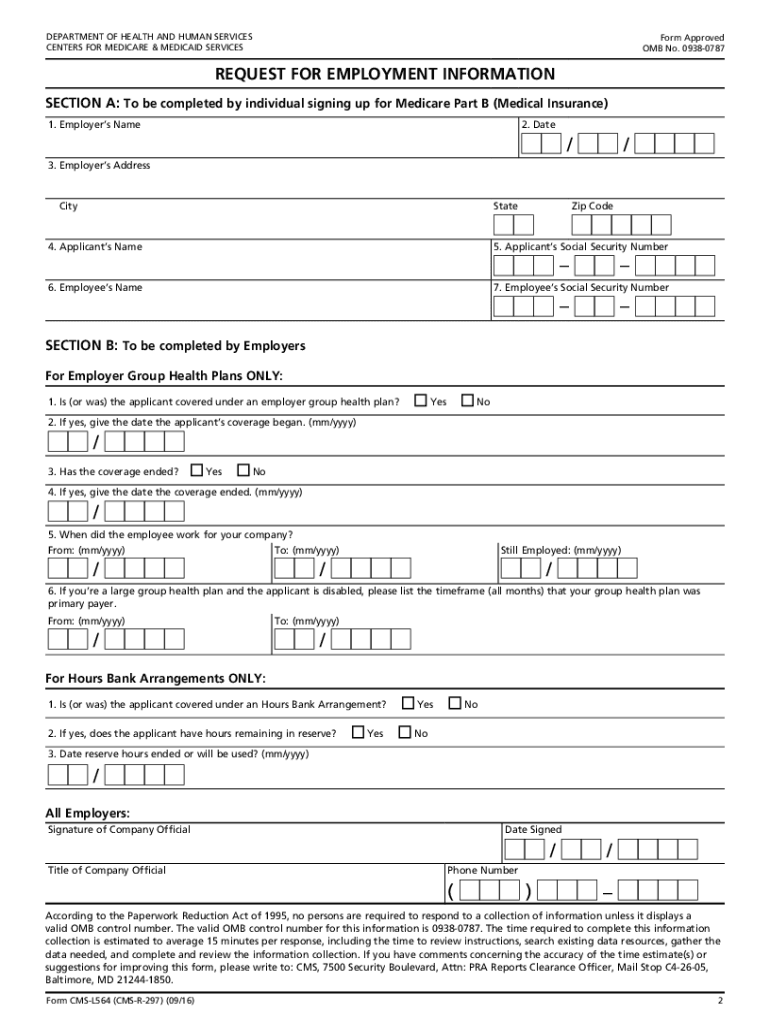
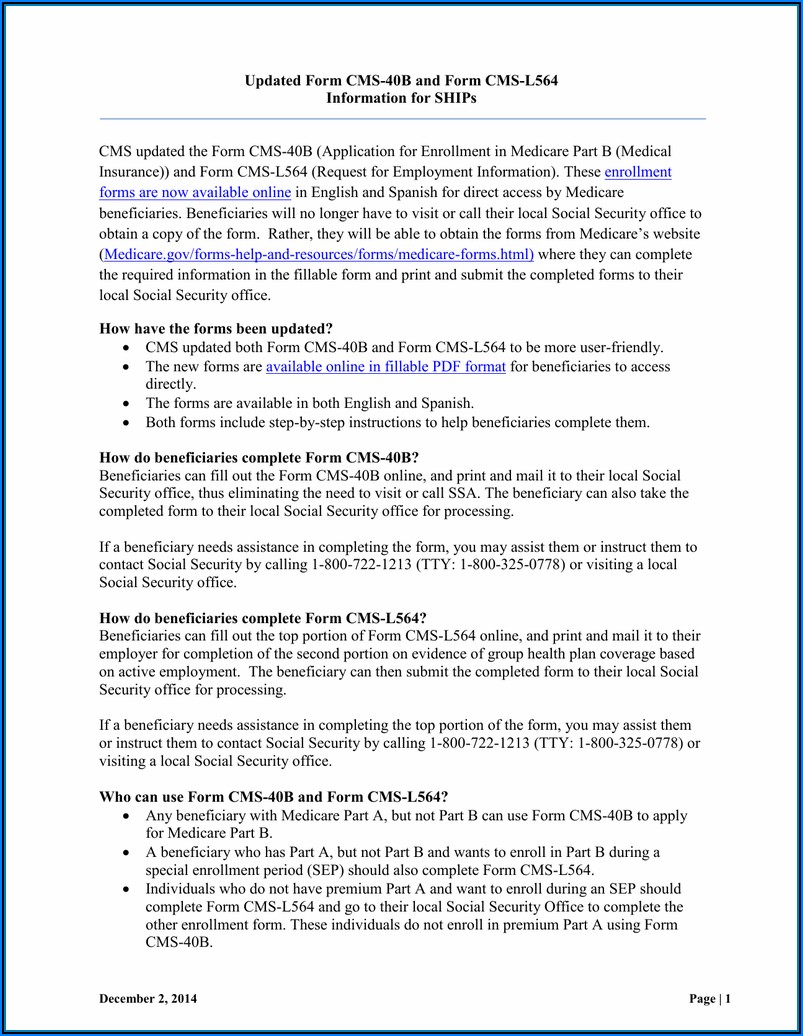
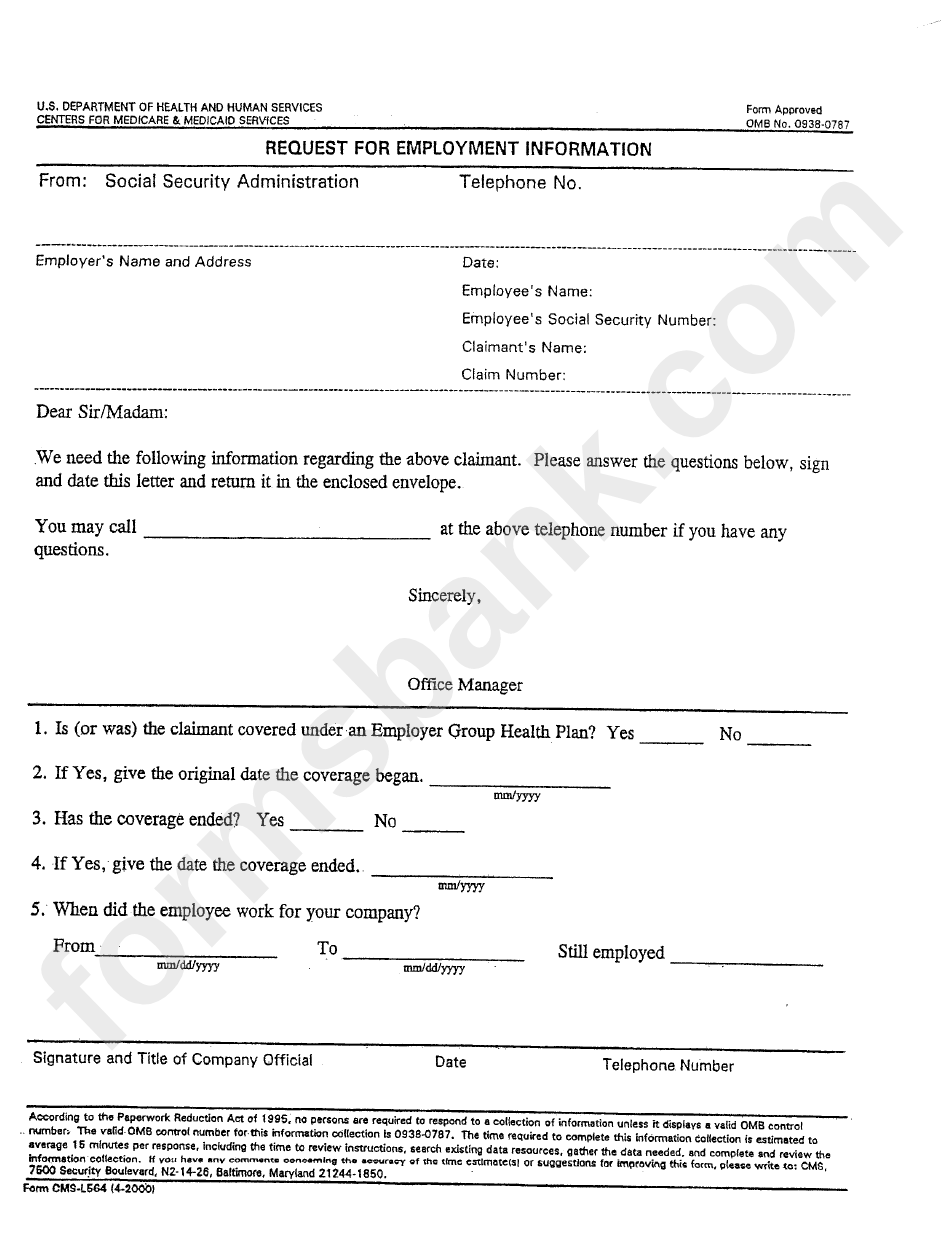
Medicare Form L564 - Social security administration telephone number: The person applying for medicare completes all of section a. The employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment. Web cms forms list. The applicant completes section a and the employer, the ghp or lghp completes section b of the form. This information is needed to process your medicare enrollment application. Giving the social security administration proof you’re eligible to sign up for part b if: Send your completed and signed application to your local social security office. Department of health and human services centers for medicare & medicaid services form approved omb no. Write the name of your employer.
Write the date that you’re filling out the request for employment. Send your completed and signed application to your local social security office. Social security administration telephone number: Giving the social security administration proof you’re eligible to sign up for part b if: You retired within the last 8 months. The employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment. You may also use the search feature to more quickly locate information for a specific form number or form title. The person applying for medicare completes all of section a. Web cms forms list. The following provides access and/or information for many cms forms.
Send your completed and signed application to your local social security office. The person applying for medicare completes all of section a. The employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment. The applicant completes section a and the employer, the ghp or lghp completes section b of the form. Social security administration telephone number: The information provided in section b is the evidence of ghp or lghp coverage. Write the date that you’re filling out the request for employment. The following provides access and/or information for many cms forms. This information is needed to process your medicare enrollment application. Web this form is used for proof of group health care coverage based on current employment.
Top Form Cmsl564 Templates free to download in PDF format
Department of health and human services centers for medicare & medicaid services form approved omb no. You retired within the last 8 months. Social security administration telephone number: You may also use the search feature to more quickly locate information for a specific form number or form title. The information provided in section b is the evidence of ghp or.
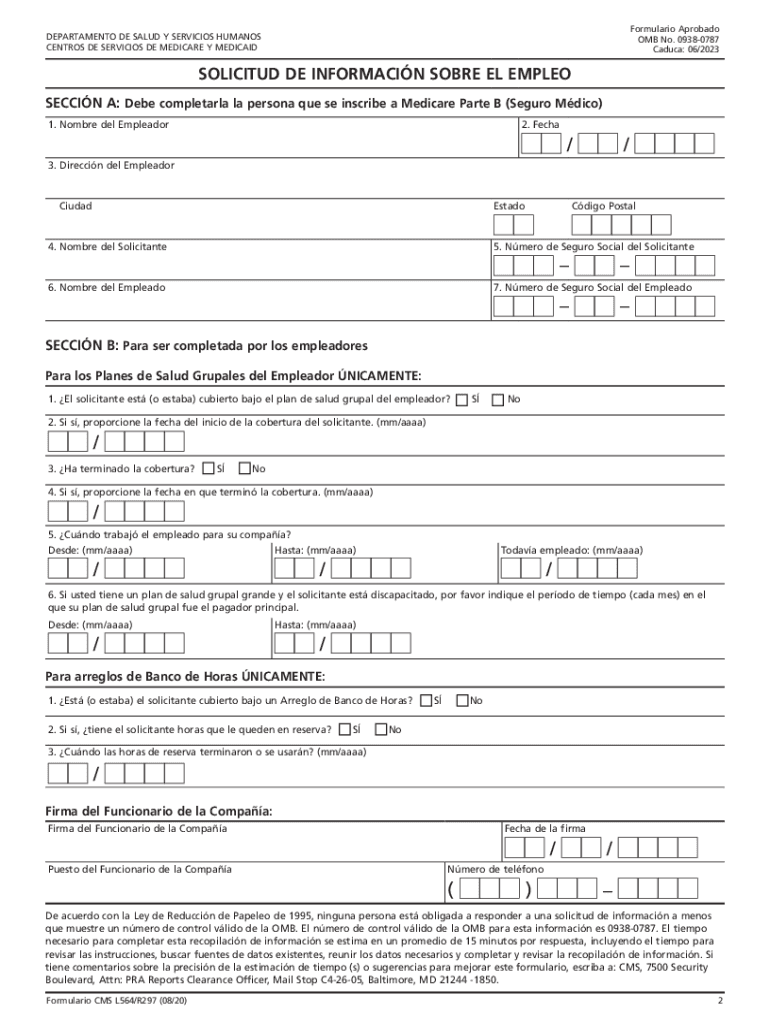
SOLICITUD DE INFORMACIN SOBRE EL EMPLEO. Formulario CMS L564/R297
You retired within the last 8 months. Send your completed and signed application to your local social security office. Write the date that you’re filling out the request for employment. Department of health and human services centers for medicare & medicaid services form approved omb no. Web this form is used for proof of group health care coverage based on.
20162021 Form CMSL564 Fill Online, Printable, Fillable, Blank pdfFiller
Write the name of your employer. The person applying for medicare completes all of section a. Web this form is used for proof of group health care coverage based on current employment. The employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment. This information is needed to process your.
Medicare Part B Form Cms L564 Form Resume Examples MeVRB6DzVD
This information is needed to process your medicare enrollment application. The person applying for medicare completes all of section a. The following provides access and/or information for many cms forms. Send your completed and signed application to your local social security office. You retired within the last 8 months.
Form CmsL564 Request For Employment Information printable pdf download
Department of health and human services centers for medicare & medicaid services form approved omb no. The information provided in section b is the evidence of ghp or lghp coverage. Send your completed and signed application to your local social security office. The person applying for medicare completes all of section a. Giving the social security administration proof you’re eligible.

Medicare Part B Application Form Cms L564 Form Resume Examples
Write the name of your employer. The person applying for medicare completes all of section a. The following provides access and/or information for many cms forms. Web this form is used for proof of group health care coverage based on current employment. Giving the social security administration proof you’re eligible to sign up for part b if:
Medicare Part B Application Form Cms L564 Form Resume Examples
Giving the social security administration proof you’re eligible to sign up for part b if: This information is needed to process your medicare enrollment application. The person applying for medicare completes all of section a. The employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment. Send your completed and.

Cms L564 Printable Form Master of Documents
Write the date that you’re filling out the request for employment. You may also use the search feature to more quickly locate information for a specific form number or form title. The person applying for medicare completes all of section a. The following provides access and/or information for many cms forms. Web cms forms list.
Printable Medicare Application Form Form Resume Examples GxKkWqeK7A
Write the name of your employer. This information is needed to process your medicare enrollment application. Send your completed and signed application to your local social security office. Write the date that you’re filling out the request for employment. Giving the social security administration proof you’re eligible to sign up for part b if:
Application For Medicare Part B Employer Form Form Resume Examples
Write the name of your employer. Web cms forms list. This information is needed to process your medicare enrollment application. Send your completed and signed application to your local social security office. Department of health and human services centers for medicare & medicaid services form approved omb no.
The Following Provides Access And/Or Information For Many Cms Forms.
The employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment. Send your completed and signed application to your local social security office. The person applying for medicare completes all of section a. You retired within the last 8 months.
The Applicant Completes Section A And The Employer, The Ghp Or Lghp Completes Section B Of The Form.
You may also use the search feature to more quickly locate information for a specific form number or form title. Write the name of your employer. The information provided in section b is the evidence of ghp or lghp coverage. Social security administration telephone number:
Department Of Health And Human Services Centers For Medicare & Medicaid Services Form Approved Omb No.
Web cms forms list. Write the date that you’re filling out the request for employment. Giving the social security administration proof you’re eligible to sign up for part b if: This information is needed to process your medicare enrollment application.