Sample Cms 1500 Form Completed
Sample Cms 1500 Form Completed - Sign up to get the latest information about your choice of cms topics. By most private insurance companies. In addition, a copy of the primary payer’s explanation of benefits (eob) notice must be Insured’s name (last name, first name, middle initial) 7. You can decide how often to. The center of medicaid and medicare services (cms) form 1500 is used to bill sfhp for medical services. Number (for program in item 1) 4. Interact with image for a magnified view. All items must be completed unless otherwise noted in these instructions. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim.
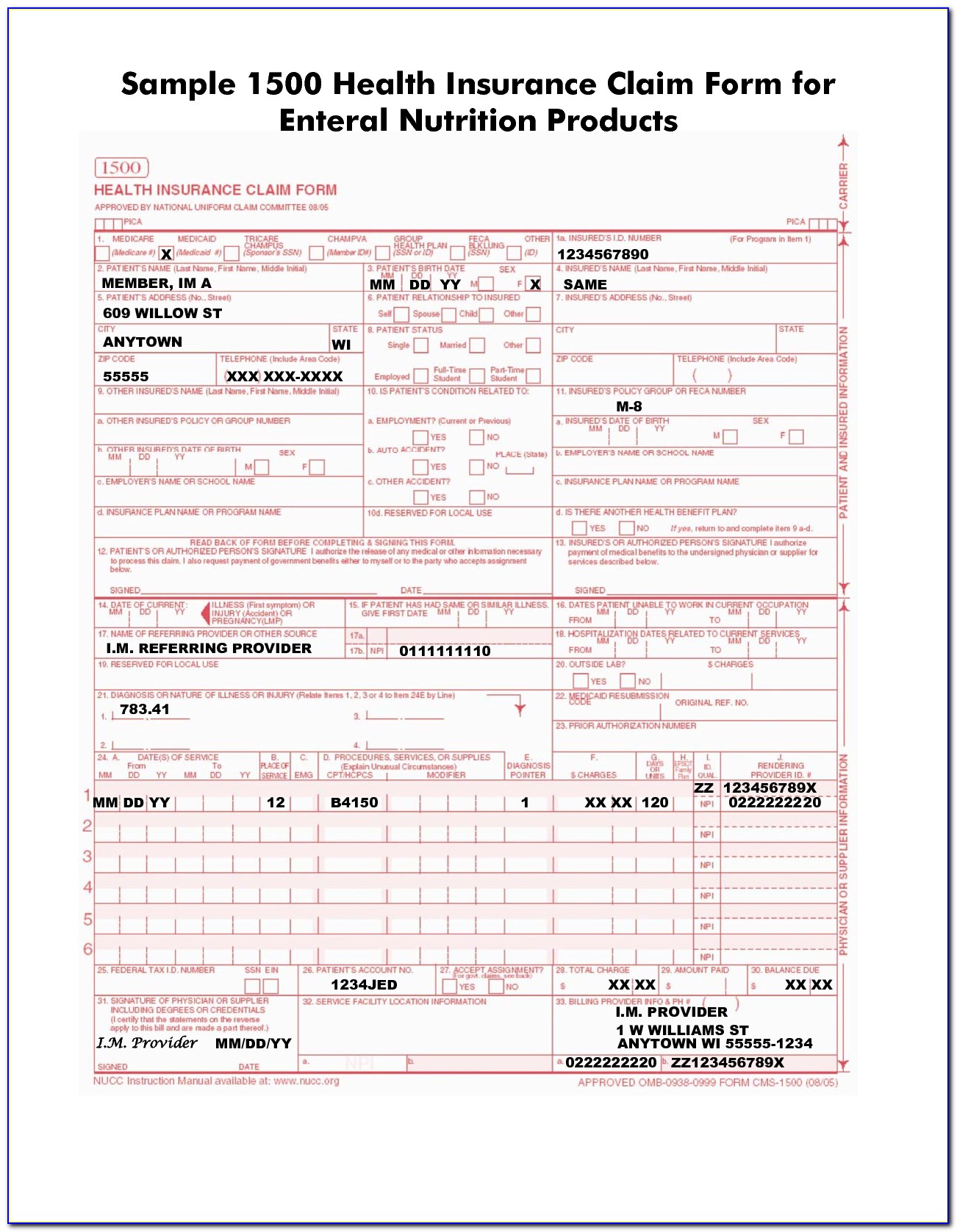
It can be purchased in any version required by calling the u.s. You may also click in any field for more detailed instructions. The uniform claim task force introduced the form in the 1980s in an effort to standardize claims nationally, writes webpt’s melissa hughes. Last updated wed, 04 jan 2023 13:36:02 +0000. The form is used by physicians and allied health professionals to submit claims for medical services. Enter the referring provider’s name in the name of referring provider or other source field (box 17) and the npi in the npi field (box 17b). The patient was seen for an office visit. You'll see instructions on how to complete the field. Web cms 1500 form o workers’ compensation (type 15); Sign up to get the latest information about your choice of cms topics.
O black lung (type 41); The copy below relates tothe graphic at left and is intended as general guidance for completing the form. Measures #130 and #131 (medication documentation and pain assessment) the slp. The uniform claim task force introduced the form in the 1980s in an effort to standardize claims nationally, writes webpt’s melissa hughes. Insured’s address (no., street) city state zip code telephone (include area code) 11. This form is the only version accepted by medicare. You can decide how often to. Number (for program in item 1) 4. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. It can be purchased in any version required by calling the u.s.

cms1500claimformsample CASO Document Management
Failure to follow these guidelines could cause a delay in processing, denial of the claim, or affect payment accuracy. Enter the referring provider’s name in the name of referring provider or other source field (box 17) and the npi in the npi field (box 17b). Sign up to get the latest information about your choice of cms topics. It is.

Example Cms 1500 Form Filled Out Form Resume Examples o7Y3LWkVBN
It can be purchased in any version required by calling the u.s. The copy below relates tothe graphic at left and is intended as general guidance for completing the form. For a paper claim to be considered for medicare secondary payer benefits, a policy or group number must be entered in this item. O black lung (type 41); By most.
Completed Cms 1500 Claim Form Sample Form Resume Examples K75PBGVkl2
All items must be completed unless otherwise noted in these instructions. You may also click in any field for more detailed instructions. It should be completed (generally electronically) and submitted to insurance provider in accordance with your organization's policies. Number (for program in item 1) 4. In addition, a copy of the primary payer’s explanation of benefits (eob) notice must.

Completed Cms 1500 Form Sample Form Resume Examples 9x8raJV3dR
By most private insurance companies. The uniform claim task force introduced the form in the 1980s in an effort to standardize claims nationally, writes webpt’s melissa hughes. Interact with image for a magnified view. It can be purchased in any version required by calling the u.s. For a paper claim to be considered for medicare secondary payer benefits, a policy.
Cms 1500 Medicare Attachment Formment Application Form Form Resume
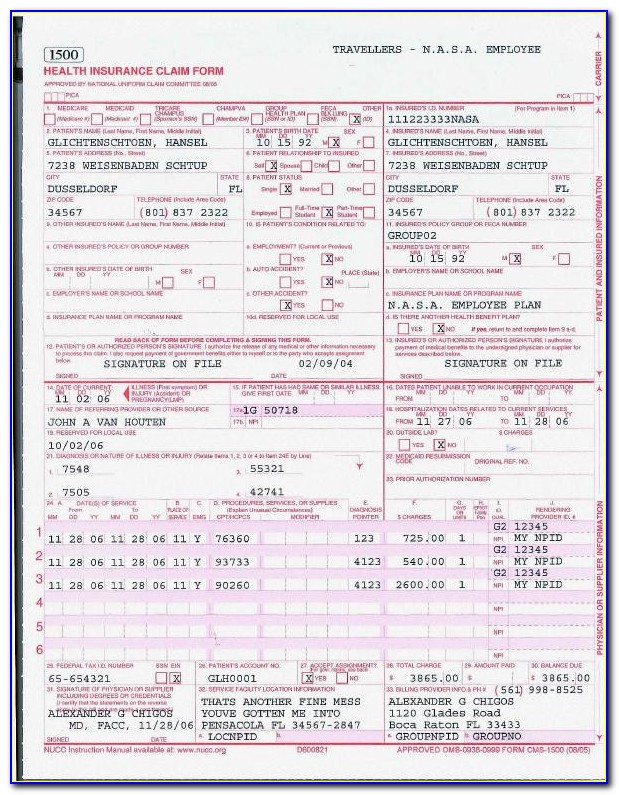
Failure to follow these guidelines could cause a delay in processing, denial of the claim, or affect payment accuracy. Number (for program in item 1) 4. By most private insurance companies. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Insured’s name (last name, first name, middle initial) 7.

Healthcare IT EMR PMS Sample CMS 1500 and UB04 Form
You can decide how often to. By most private insurance companies. Number (for program in item 1) 4. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. And o veterans benefits (type 42).
Completed Cms 1500 Form Sample Form Resume Examples 9x8raJV3dR
Web instructions for completing the cms 1500 claim form the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for medical services. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing.

Completed Cms 1500 Form Sample Form Resume Examples 9x8raJV3dR
It can be purchased in any version required by calling the u.s. Interact with image for a magnified view. Enter the referring provider’s name in the name of referring provider or other source field (box 17) and the npi in the npi field (box 17b). By most private insurance companies. Number (for program in item 1) 4.
:max_bytes(150000):strip_icc()/CMS-1500-claim-form-57a2d3a85f9b589aa99caf8b.jpg)
CMS 1500 Claim Form Versions and Tips
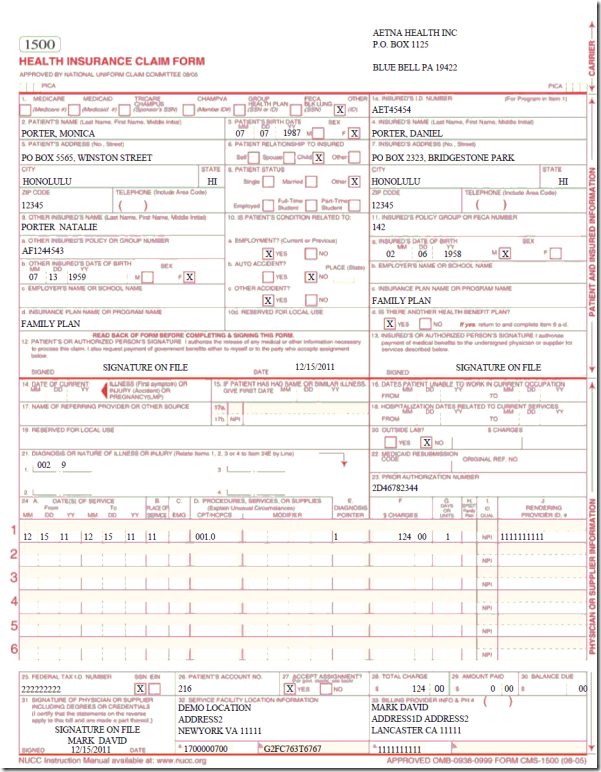
This form is the only version accepted by medicare. Web cms 1500 dynamic list information. Insured’s address (no., street) city state zip code telephone (include area code) 11. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing.
Healthcare IT EMR PMS Sample CMS 1500 and UB04 Form
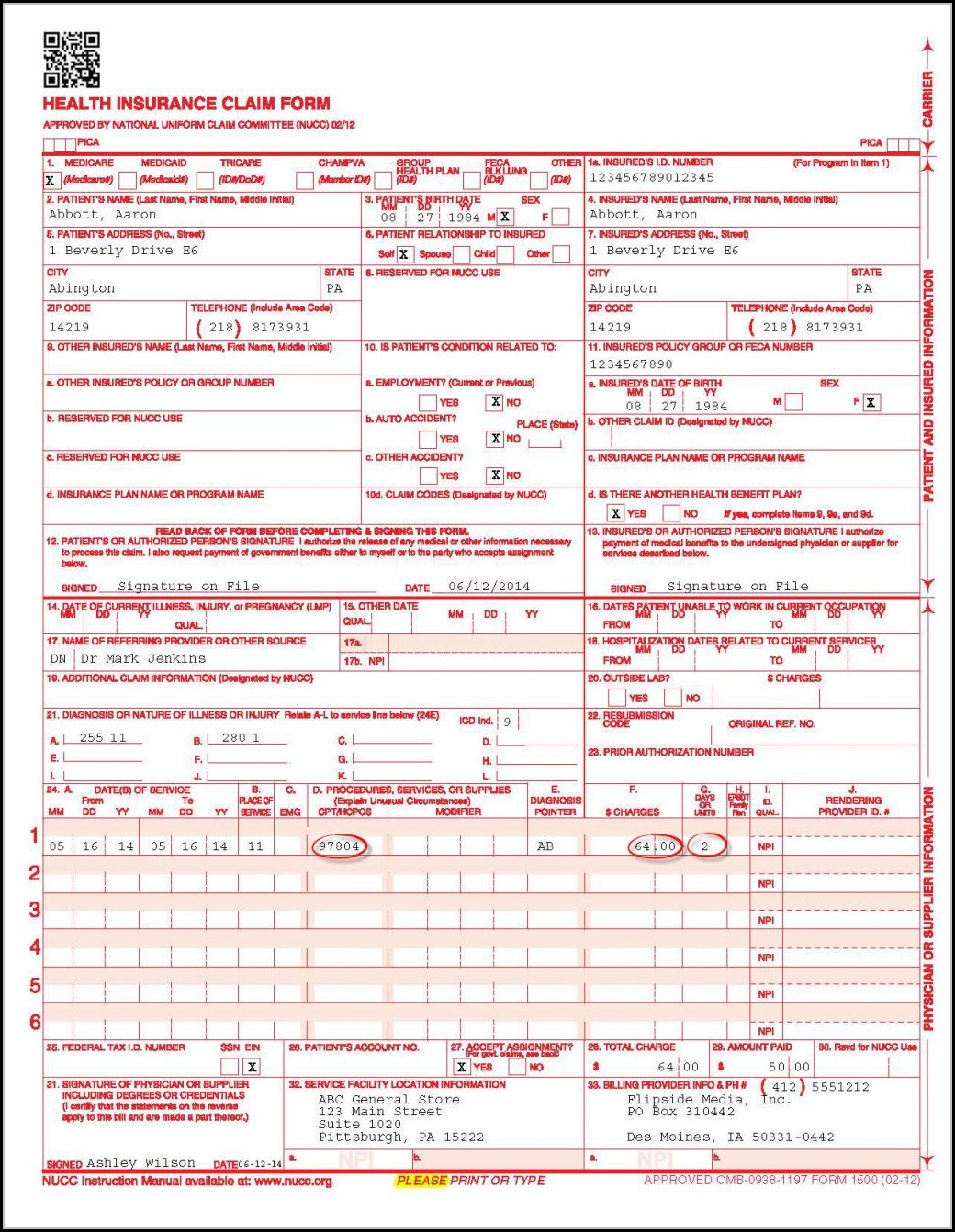
The patient was seen for an office visit. The copy below relates tothe graphic at left and is intended as general guidance for completing the form. This form is the only version accepted by medicare. Web cms 1500 form o workers’ compensation (type 15); Failure to follow these guidelines could cause a delay in processing, denial of the claim, or.
And O Veterans Benefits (Type 42).
Measures #130 and #131 (medication documentation and pain assessment) the slp. The form is used by physicians and allied health professionals to submit claims for medical services. You may also click in any field for more detailed instructions. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers.
It Is The Basic Paper Claim Form Prescribed By Many Payers For Claims Submitted By Physicians, Other Providers, And Suppliers, And In Some Cases, For Ambulance Services.
It should be completed (generally electronically) and submitted to insurance provider in accordance with your organization's policies. Web instructions for completing the cms 1500 claim form the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for medical services. Enter the referring provider’s name in the name of referring provider or other source field (box 17) and the npi in the npi field (box 17b). Insured’s name (last name, first name, middle initial) 7.
For A Paper Claim To Be Considered For Medicare Secondary Payer Benefits, A Policy Or Group Number Must Be Entered In This Item.
Last updated wed, 04 jan 2023 13:36:02 +0000. The copy below relates tothe graphic at left and is intended as general guidance for completing the form. O black lung (type 41); By most private insurance companies.
It Can Be Purchased In Any Version Required By Calling The U.s.
The form is used by physicians and allied health professionals to submit claims for medical services. Insured’s address (no., street) city state zip code telephone (include area code) 11. Sign up to get the latest information about your choice of cms topics. Insured’s policy group or feca number a.