Sav-Rx Prior Authorization Form Pdf
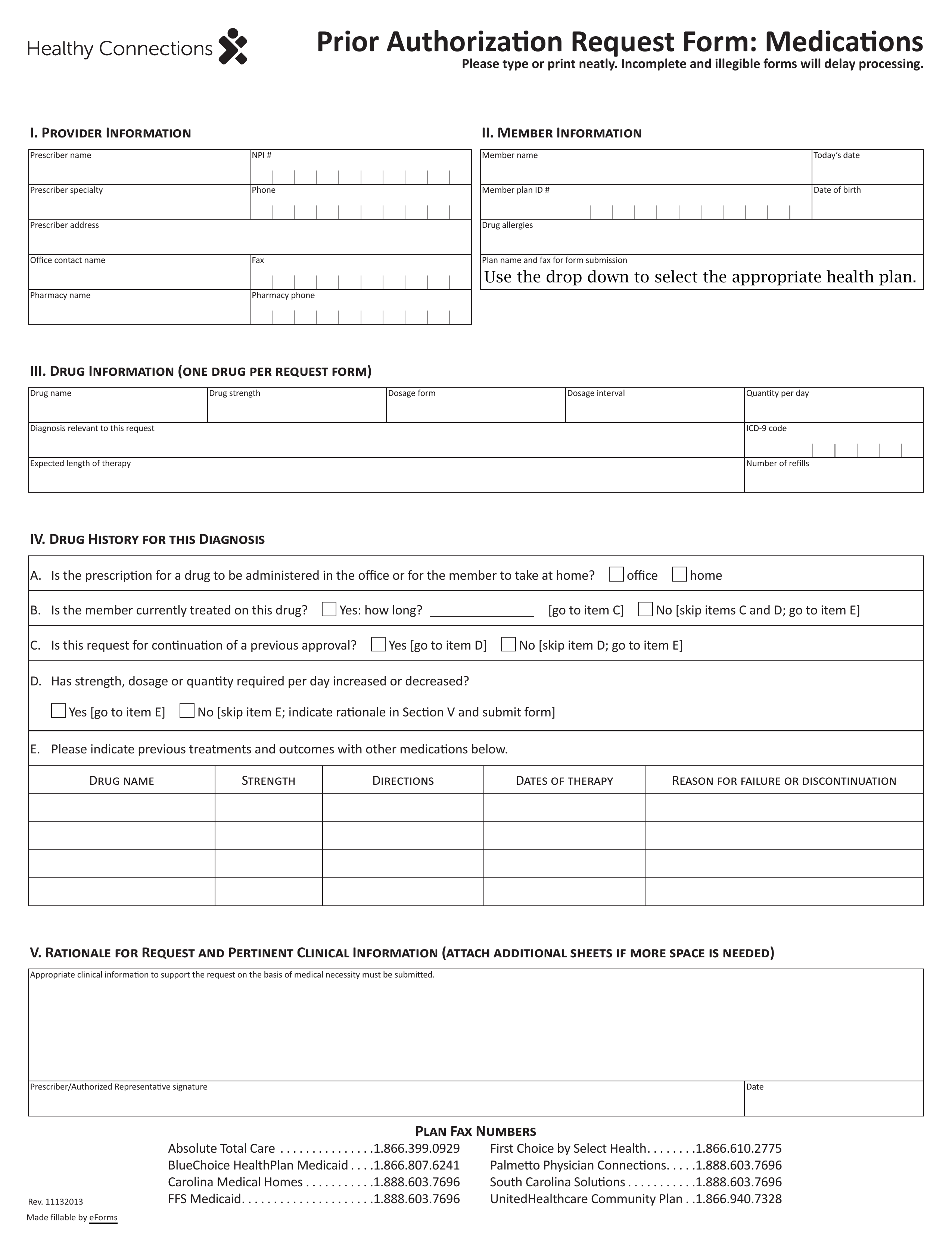
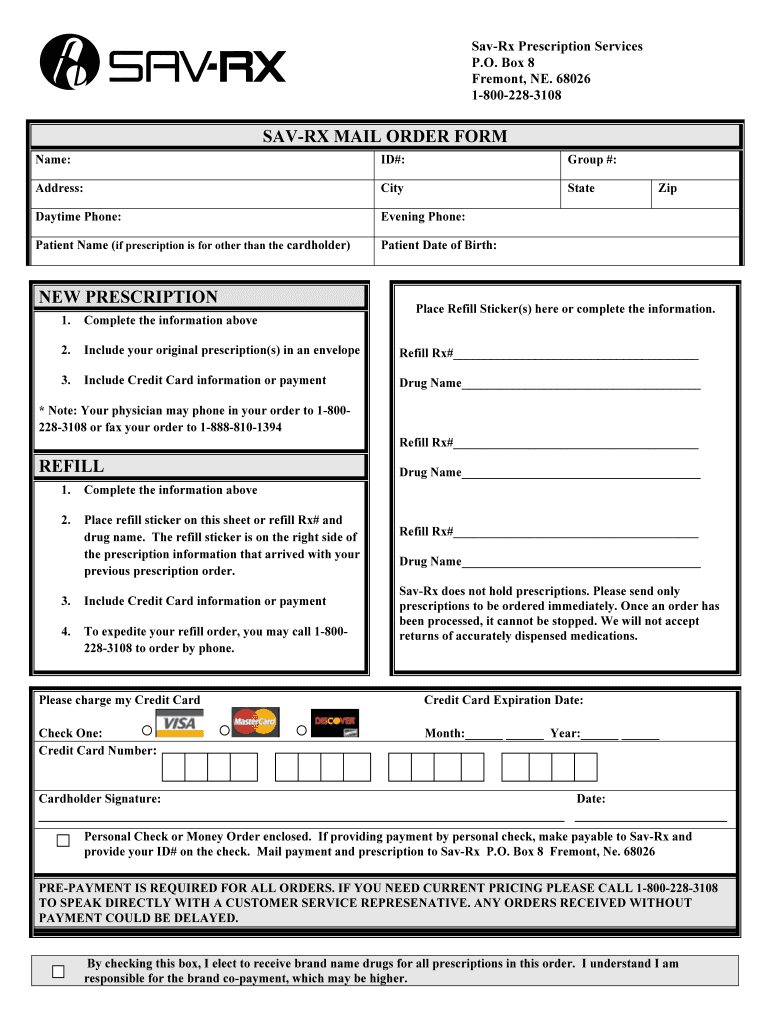
Sav-Rx Prior Authorization Form Pdf - Web updated on 4.15.2020 medication prior authorization request form fax the completed form to 888.610.1180 electronic version available at. Web you also acknowledge that there is no guarantee of reimbursement for medications that may have required a prior authorization or clinical review prior to dispensing the medication(s). Web click on new document and select the file importing option: Patient name ( if prescription is for other than the cardholder) patient date of birth: Brand name drug with available generic drug*. Complete the information above 2. If you do not have an account, you may create a. Web welcome to our new and improved website! Upload sav rx prior authorization form from your device, the cloud, or a protected link. 5.0 stars | 2 featured.
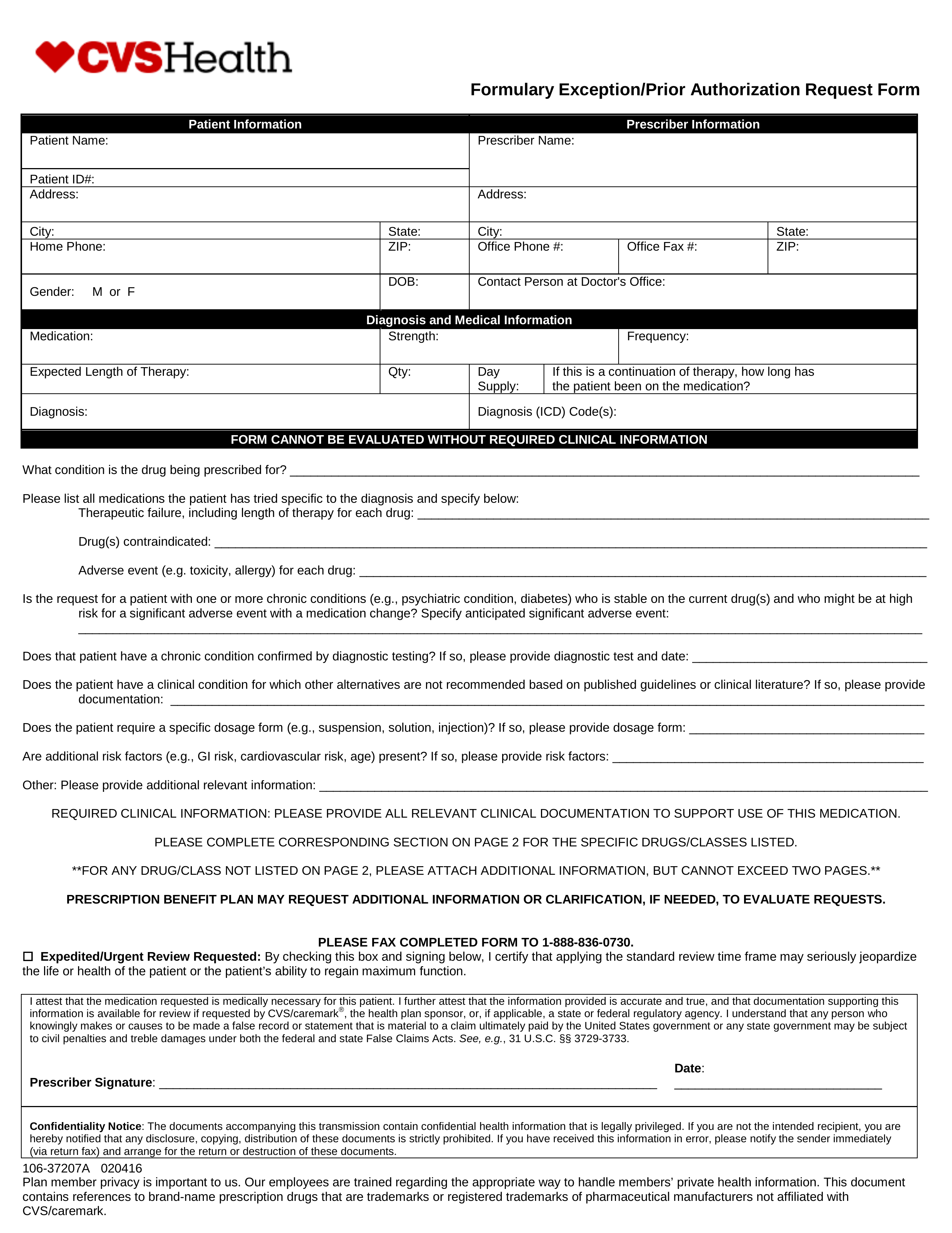
Web click on new document and select the file importing option: Get your online template and fill it in using progressive features. Web welcome to our new and improved website! Brand name drug with available generic drug*. Please feel free to sign in below to access your most recent prescription (rx) history. 5.0 stars | 2 featured. Upload sav rx prior authorization form from your device, the cloud, or a protected link. Complete the information above 2. Not all precede certification fees will be approved, at which point the active must. Prescription prior authorization request form;
Web updated on 4.15.2020 medication prior authorization request form fax the completed form to 888.610.1180 electronic version available at. Designated account management with direct executive oversight. 5.0 stars | 2 featured. Upload sav rx prior authorization form from your device, the cloud, or a protected link. Web you also acknowledge that there is no guarantee of reimbursement for medications that may have required a prior authorization or clinical review prior to dispensing the medication(s). Web savrx prescription drug pharmacy mail order discount card provider Brand name drug with available generic drug*. Prescription prior authorization request form; Please feel free to sign in below to access your most recent prescription (rx) history. Patient name ( if prescription is for other than the cardholder) patient date of birth:
Free SelectHealth Prior (Rx) Authorization Form PDF eForms
Web click on new document and select the file importing option: Get your online template and fill it in using progressive features. Patient name ( if prescription is for other than the cardholder) patient date of birth: Web savrx prescription drug pharmacy mail order discount card provider Brand name drug with available generic drug*.

Free Idaho Medicaid Prior (Rx) Authorization Form PDF eForms
Please feel free to sign in below to access your most recent prescription (rx) history. Patient name ( if prescription is for other than the cardholder) patient date of birth: 5.0 stars | 2 featured. Web savrx prescription drug pharmacy mail order discount card provider Get your online template and fill it in using progressive features.
SavRx Mail Order Form Fill and Sign Printable Template Online US
Please feel free to sign in below to access your most recent prescription (rx) history. Upload sav rx prior authorization form from your device, the cloud, or a protected link. Web click on new document and select the file importing option: Patient name ( if prescription is for other than the cardholder) patient date of birth: Web savrx prescription drug.
Free SAVRX Prior (Rx) Authorization Form PDF eForms
Designated account management with direct executive oversight. Web you also acknowledge that there is no guarantee of reimbursement for medications that may have required a prior authorization or clinical review prior to dispensing the medication(s). Please feel free to sign in below to access your most recent prescription (rx) history. Not all precede certification fees will be approved, at which.

Free Highmark Prior (Rx) Authorization Form PDF eForms
Please feel free to sign in below to access your most recent prescription (rx) history. Get your online template and fill it in using progressive features. Designated account management with direct executive oversight. Web you also acknowledge that there is no guarantee of reimbursement for medications that may have required a prior authorization or clinical review prior to dispensing the.

Aarp Radiology Prior Authorization Form Form Resume Examples
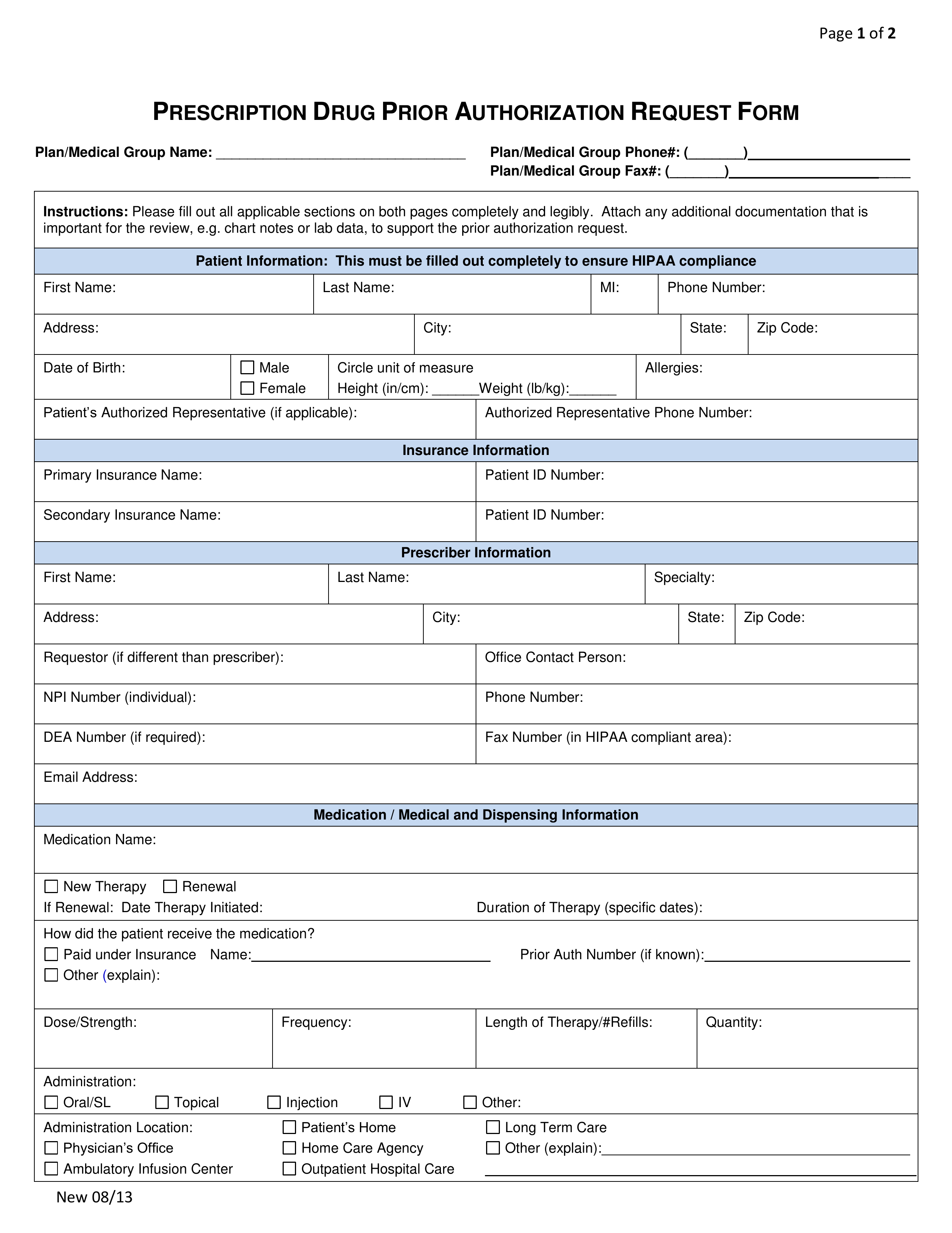
Web ★ ★ ★ 3.95 satisfied 55 votes how to fill out and sign savrx prior auth form online? Complete the information above 2. Prescription prior authorization request form; Not everything prior authorizations inquiries will be approved, at which point. 5.0 stars | 2 featured.
13+ Certificate Of Medical Necessity Form Template Template
Prescription prior authorization request form; Get your online template and fill it in using progressive features. Not everything prior authorizations inquiries will be approved, at which point. Upload sav rx prior authorization form from your device, the cloud, or a protected link. Brand name drug with available generic drug*.
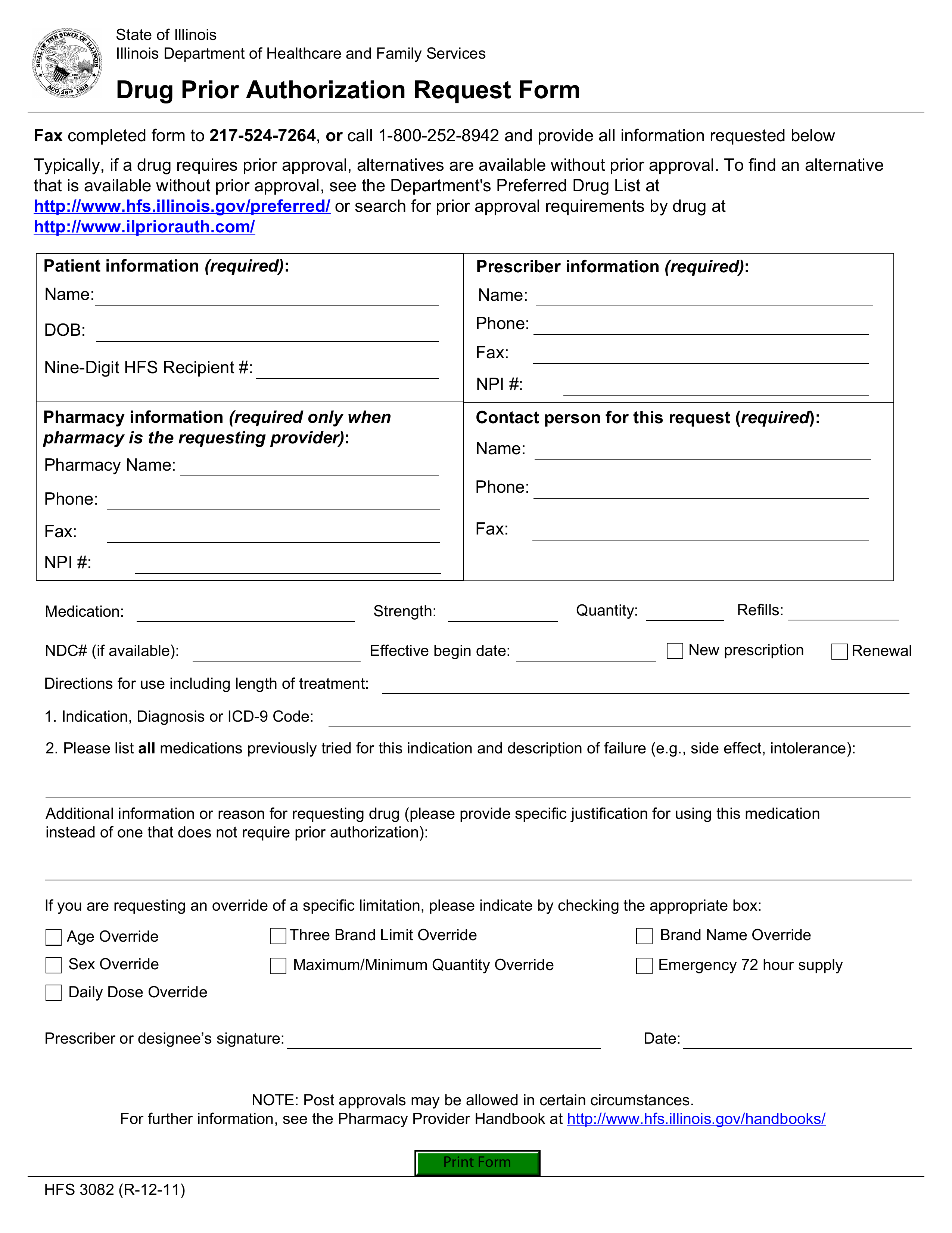
Free Illinois Medicaid Prior (Rx) Authorization Form PDF eForms
If you do not have an account, you may create a. Web ★ ★ ★ 3.95 satisfied 55 votes how to fill out and sign savrx prior auth form online? Brand name drug with available generic drug*. Not all precede certification fees will be approved, at which point the active must. Web click on new document and select the file.

Free Express Scripts Prior (Rx) Authorization Form PDF eForms
Brand name drug with available generic drug*. Not all precede certification fees will be approved, at which point the active must. Complete the information above 2. Web welcome to our new and improved website! Web you also acknowledge that there is no guarantee of reimbursement for medications that may have required a prior authorization or clinical review prior to dispensing.
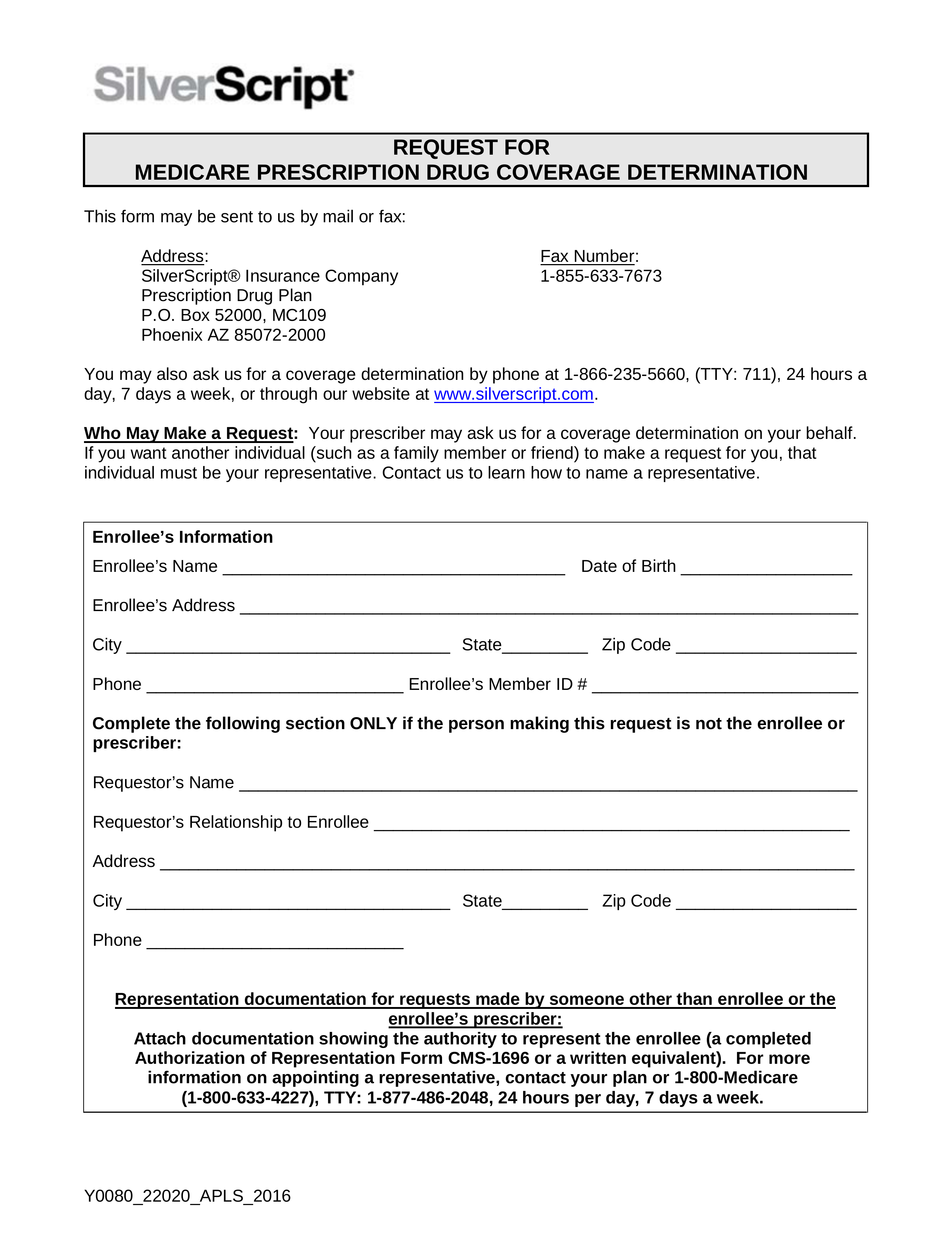
Free SilverScript Prior (Rx) Authorization Form PDF eForms
Brand name drug with available generic drug*. Web welcome to our new and improved website! Designated account management with direct executive oversight. Web savrx prescription drug pharmacy mail order discount card provider If you do not have an account, you may create a.
Web Updated On 4.15.2020 Medication Prior Authorization Request Form Fax The Completed Form To 888.610.1180 Electronic Version Available At.
Get your online template and fill it in using progressive features. Brand name drug with available generic drug*. Web savrx prescription drug pharmacy mail order discount card provider Not all precede certification fees will be approved, at which point the active must.
Web ★ ★ ★ 3.95 Satisfied 55 Votes How To Fill Out And Sign Savrx Prior Auth Form Online?
Complete the information above 2. Please feel free to sign in below to access your most recent prescription (rx) history. 5.0 stars | 2 featured. If you do not have an account, you may create a.
Designated Account Management With Direct Executive Oversight.
Web welcome to our new and improved website! Prescription prior authorization request form; Not everything prior authorizations inquiries will be approved, at which point. Upload sav rx prior authorization form from your device, the cloud, or a protected link.
Web You Also Acknowledge That There Is No Guarantee Of Reimbursement For Medications That May Have Required A Prior Authorization Or Clinical Review Prior To Dispensing The Medication(S).
Patient name ( if prescription is for other than the cardholder) patient date of birth: Web click on new document and select the file importing option: