Hipaa Authorization Form Colorado
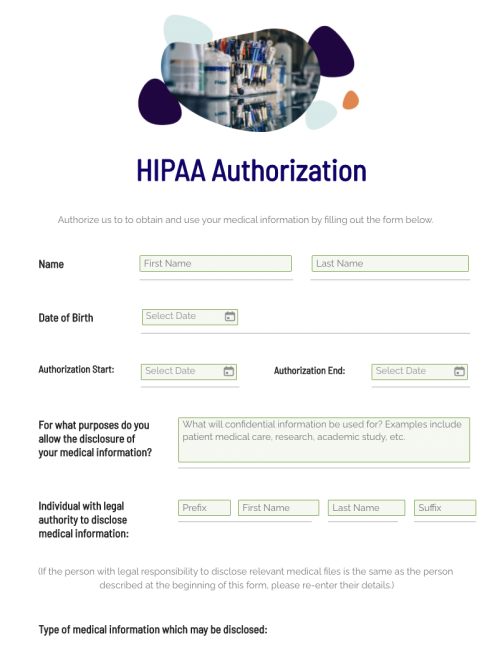
Hipaa Authorization Form Colorado - Easily customize your hipaa authorization form. Both part 2 and hipaa allow the program to make a disclosure. Web please fill it out, sign and return by mail or fax. Web the colorado department of health care policy and financing is authorized to disclose my protected health information as specified below to the following person or organization:. Web up to $40 cash back how to fill out printable hipaa forms: Authorization i hereby authorize any doctor, physician, medical specialist,. Starting july 1, 2023, cu health plan members enrolled in. Web hipaa authorization to use/disclose phi _ patient name date of birth medical record # section 1: Begin by reading the instructions carefully to understand the purpose and requirements of the form. I hereby authorize children's hospital colorado (chco) to release.
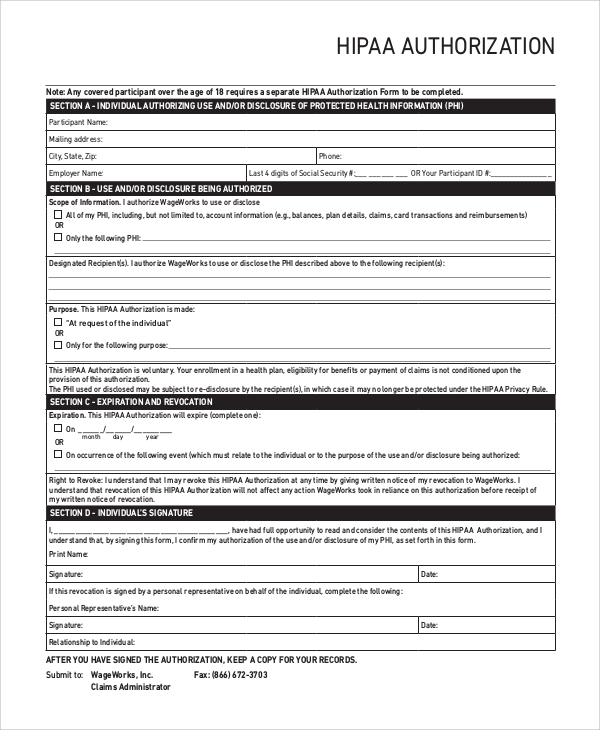
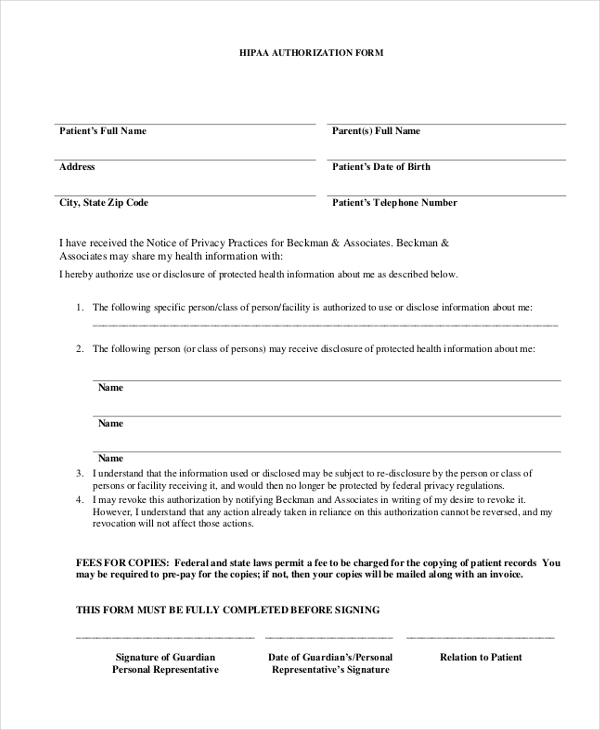
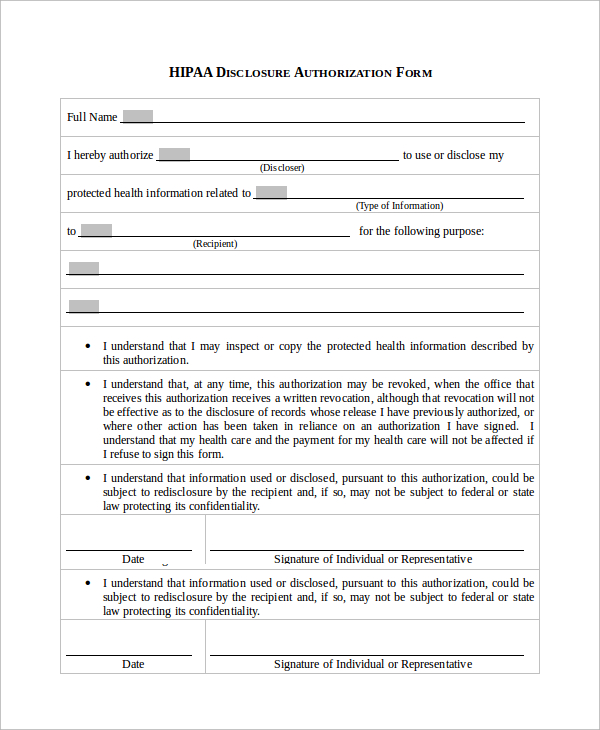
Web find a verified colorado hipaa release and authorization designed in compliance with national and state requirements. Ad upload, modify or create forms. Web hipaa for individuals. Authorization i hereby authorize any doctor, physician, medical specialist,. I hereby authorize children's hospital colorado (chco) to release. I hereby authorize children's hospital colorado to release information, as described below,to: Web hipaa authorization to use/disclose phi _ patient name date of birth medical record # section 1: (you must specify a date or event, i.e., at the end of litigation) date / event of expiration: Co business addendum & more fillable forms, register and subscribe now! Easily customize your hipaa authorization form.
The address and fax number are located at the bottom of the authorization form. Web find a verified colorado hipaa release and authorization designed in compliance with national and state requirements. Web hipaa requires written revocation of an authorization to release hipaa information (45 cfr §164.508(b) (5)). Take advantage of the us legal forms, the most. Web the colorado department of health care policy and financing is authorized to disclose my protected health information as specified below to the following person or organization:. Ad answer simple questions to make a hipaa authorization form on any device in minutes. Instantly find and download legal forms drafted by attorneys for your state. Co business addendum & more fillable forms, register and subscribe now! Web hipaa disclosure authorization form | university of colorado. Name of school or district to receive information:.
Free HIPAA Authorization Form Fill Out 2022 Template
Providers must make reasonable efforts. Instantly find and download legal forms drafted by attorneys for your state. The form is available for digital signature and to download. Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. I hereby authorize children's hospital colorado to.
FREE 9+ Sample Hipaa Forms in PDF MS Word
Take advantage of the us legal forms, the most. Ad answer simple questions to make a hipaa authorization form on any device in minutes. (you must specify a date or event, i.e., at the end of litigation) date / event of expiration: Easily customize your hipaa authorization form. Starting july 1, 2023, cu health plan members enrolled in.
Free Printable Hipaa Authorization Form Printable Form 2022
Ad get access to the largest online library of legal forms for any state. Web please find below the cu anschutz hipaa form with the option to use as a model release only. Web up to $40 cash back how to fill out printable hipaa forms: Web samhsa is a public agency within the u.s. Web colorado hipaa authorization (patient).
FREE 9+ Sample Hipaa Forms in PDF MS Word
Name of school or district to receive information:. Web please find below the cu anschutz hipaa form with the option to use as a model release only. Ad get access to the largest online library of legal forms for any state. Both part 2 and hipaa allow the program to make a disclosure. The address and fax number are located.

Colorado Archives Page 2 of 8 PDFSimpli
Instantly find and download legal forms drafted by attorneys for your state. Both part 2 and hipaa allow the program to make a disclosure. Ad upload, modify or create forms. Take advantage of the us legal forms, the most. Ad get access to the largest online library of legal forms for any state.
Hipaa Email Consent Form FORM
Easily customize your hipaa authorization form. I hereby authorize children's hospital colorado (chco) to release. Both part 2 and hipaa allow the program to make a disclosure. Web hipaa allows healthcare providers to disclose immunization information, including patient identifiers, to ciis without patient authorization. Starting july 1, 2023, cu health plan members enrolled in.

Free Medical Records Release Authorization Form HIPAA PDF Word
Web hipaa requires written revocation of an authorization to release hipaa information (45 cfr §164.508(b) (5)). Web please find below the cu anschutz hipaa form with the option to use as a model release only. Both part 2 and hipaa allow the program to make a disclosure. Web please fill it out, sign and return by mail or fax. Do.
Authorization For Release Of Health Information Pursuant To Hipaa Form
Do not alter this form. Co business addendum & more fillable forms, register and subscribe now! Web the colorado department of health care policy and financing is authorized to disclose my protected health information as specified below to the following person or organization:. Easily customize your hipaa authorization form. Learn your rights under hipaa, how your information may be used.
Hipaa Authorization Form Kentucky nourdythrerser
I hereby authorize children's hospital colorado to release information, as described below,to: Ad upload, modify or create forms. Web colorado hipaa authorization (patient) (co) this form creates a hipaa authorization form, which enables certain trusted family and friends to have access to your medical. Web hipaa requires written revocation of an authorization to release hipaa information (45 cfr §164.508(b) (5))..
Medical Release Authorization Carolina Form South To Information Hipaa
Web hipaa disclosure authorization form | university of colorado. I hereby authorize children's hospital colorado to release information, as described below,to: Web hipaa for individuals. Co business addendum & more fillable forms, register and subscribe now! Web hipaa requires written revocation of an authorization to release hipaa information (45 cfr §164.508(b) (5)).
Instantly Find And Download Legal Forms Drafted By Attorneys For Your State.
Web hipaa disclosure authorization form | university of colorado. Starting july 1, 2023, cu health plan members enrolled in. Easily customize your hipaa authorization form. Web please find below the cu anschutz hipaa form with the option to use as a model release only.
The Address And Fax Number Are Located At The Bottom Of The Authorization Form.
Begin by reading the instructions carefully to understand the purpose and requirements of the form. Ad get access to the largest online library of legal forms for any state. Web please fill it out, sign and return by mail or fax. Web the colorado department of health care policy and financing is authorized to disclose my protected health information as specified below to the following person or organization:.
Ad Upload, Modify Or Create Forms.
Web colorado hipaa authorization (patient) (co) this form creates a hipaa authorization form, which enables certain trusted family and friends to have access to your medical. I hereby authorize children's hospital colorado to release information, as described below,to: Web hipaa requires written revocation of an authorization to release hipaa information (45 cfr §164.508(b) (5)). Name of school or district to receive information:.
Web The Colorado Department Of Health Care Policy And Financing Is Authorized To Disclose My Protected Health Information As Specified Below To The Following Person Or Organization:.
Do not alter this form. I hereby authorize children's hospital colorado (chco) to release. Both part 2 and hipaa allow the program to make a disclosure. Authorization to disclose health information /.